Case Report
2016
March
Volume : 4
Issue : 1
Spontaneous transanal externalization of ventriculoperitoneal shunt
Raghavendra H, Swetha Pendyala, Trivedi Punit, Manas Kumar Panigraghi
Pdf Page Numbers :- 8-10
Raghavendra H1,*, Swetha Pendyala1, Trivedi Punit1, and Manas Kumar Panigraghi1
1Dept of Neurosurgery, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India
*Corresponding author: Raghavendra H, Krishna Institute of Medical Sciences, Minister Road, Secunderabad-500003, Telangana, India. Email: raghavendra.harpanahalli@gmail.com
Received 2 October 2015; Revised 27 November 2015; Accepted 9 December 2015; Published 18 December 2015
Citation: Raghavendra H, Pendyala S, Punit T, Panigraghi MK. Spontaneous transanal externalization of ventriculoperitoneal shunt. J Med Sci Res. 2016; 4(1):8-10. DOI: http://dx.doi.org/10.17727/JMSR.2016/4-003
Copyright: © 2016 Raghavendra H, et al. Published by KIMS Foundation and Research Center. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Aim of this paper is to report a case of spontaneous externalization of Ventriculoperitoneal shunt tube through anus in an eighteen months female child (k/c/o Dandy-Walker malformation) treated with placement of ventriculoperitoneal shunt for hydrocephalus. The exact cause of such externalization is not known. Unusual migration of distal catheter tip of VP shunt is a rare and bowel perforation is reported to occur between 0.1% and 0.7%. In view of the potential risk for meningitis prompt and aggressive management is essential to avoid morbidity and mortality.
Keywords: Transanal externalization; ventriculoperitoneal; Dandy-Walker; hydrocephalus
Full Text
Ventriculoperitoneal (VP) shunting used in the treatment for hydrocephalus is associated with several complications with a reported incidence of 5–47% of cases [1]. Bowel perforation and spontaneous externalization of the lower end of the tube through the anal opening is a rare and unusual complication of the ventriculoperitoneal shunt [2]. Here, we report a case of transanal externalization of VP shunt catheter with a review of pertinent literature.
Case report
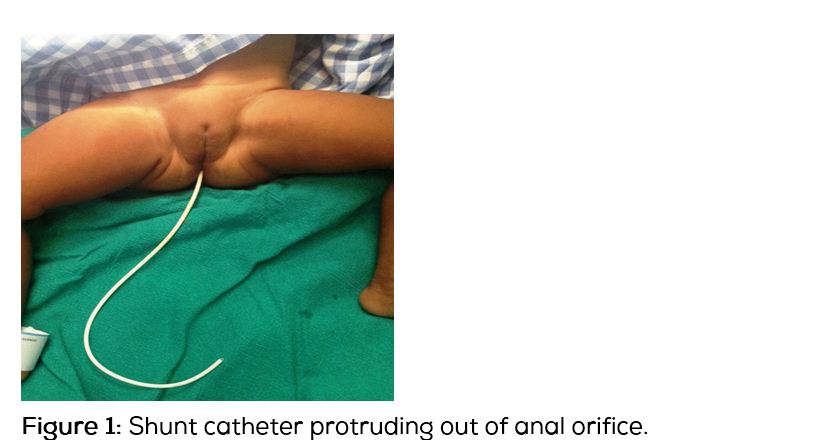
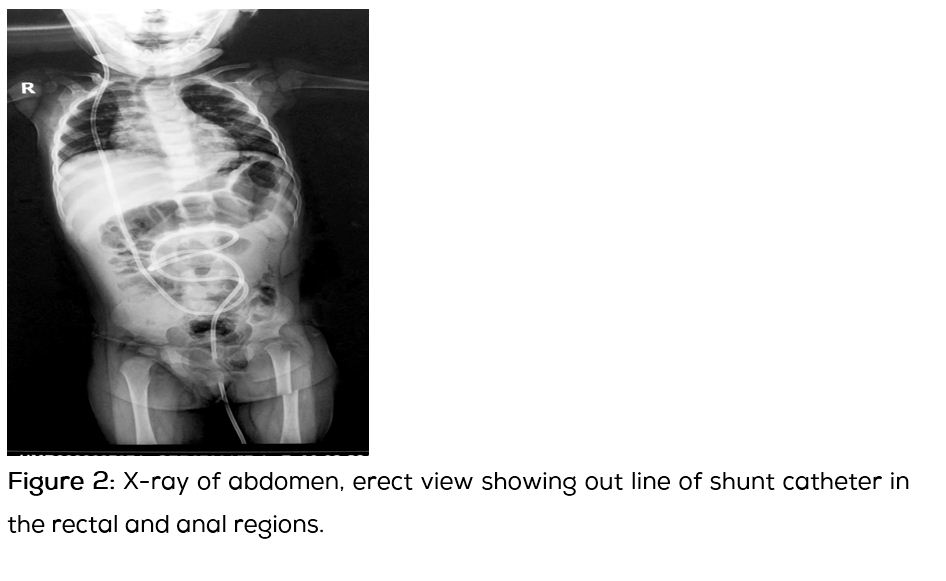
An eighteen -month-old female child had undergone a right sided VP shunt (Chhabra-slit-in-spring silicone shunt) procedure 6 months back for congenital hydrocephalus with Dandy-Walker malformation. She presented with complaints of protrusion of a white tube per anus on defecation one day duration with clear fluid dripping from it (Figure 1). On examination, the child was a febrile, alert, shrunken anterior fontanelle and had no neck rigidity, and the abdomen was soft. On rectal examination, there was a white tube coming from beyond the reach of finger. X-ray of the abdomen showed the course of the shunt tube toward the rectum and anal opening and did not reveal any evidence of gas under diaphragm (Figure 2). The child was operated and the cranial end was removed through a small incision behind the ear. The distal tube was extracted per rectum (to avoid contamination) and cerebral reservoir was placed. On 1st post operative day, anterior fontanelle became full for external ventricular catheter was connected. Proximal tube was cultured and was found to be the sterile. A revision shunt was done on the opposite side after 2 weeks.
Discussion
VP shunt is an established method of diverting CSF for the management of hydrocephalus [3]. The peritoneal end of the VP shunt has been associated with complications such as mechanical blockade by omentum leading to shunt failure, pseudocyst formation, intestinal volvulus, inguinal hernia, perforations of hollow viscus, penetration into solid organs & abdominal wall and protrusion outside body [4]. Shunt migration into stomach, bowel, liver, chest, jugular vein, anus, vagina, and scrotum has been reported previously. Migration of the lower end of the shunt catheter occurs without any recognizable cause. Distal shunt migration has been reported in as many 10% of these cases [5].
Abdominal complications account for about 25% of the complications caused by ventriculoperitoneal shunt insertion. Bowel perforation occurs between 0.1% and 0.7% of the times which may lead to significant morbidity and mortality due to peritonitis and/ or meningoventriculitis [6]. Thin bowel wall in children, sharp and stiff end of the VP shunt, use of trocar by some surgeons, chronic irritation by the shunt, previous surgery, infection and silicone allergy are some of the factors responsible for bowel perforation by ventriculoperitoneal shunt.
Catheter-induced gut perforations have been reported previously in the literature (at least 119 cases), with most common site being colon (70%), followed by the stomach (16%), and small bowel (14%). Factors like poor host immunity & bioreactivity of shunt components contribute to shunt extrusion [7]. There is not an obvious relationship between the length of the distal end of the shunt and perforation rates. Vuyyuru et al., reported that malnutrition and a former abdominal surgery may increase the risk of migration due to adhesions arising from infection [8].
Most patients with abdominal complications are asymptomatic. Fibrous tract formed at the perforated site usually seals the perforation, preventing spillage of faecal matter into the peritoneum, preventing peritonitis and delaying the correct diagnosis until a later stage at which ventriculitis or central nervous system infection has been fully established. In patients with the transanal protrusion of a VP shunt catheter, the diagnosis is obvious. The period between shunt placing and the protrusion of the catheter from the anus ranges from 2 to 20 months [9].
Management involves prompt removal of shunt, intravenous antibiotics, an adequate recovery gap so that cerebrospinal fluid culture is sterile and then followed by shunt replacement on opposite side. During the interval which is about 3-4 weeks, the patient can be kept on cerebral dehydrants to limit the increasing hydrocephalus. In a patient with simple bowel perforation and no other complications, a formal laparotomy is not required while in patients with intra-abdominal complications, urgent laparotomy should be undertaken.
Conclusion
Anal protrusion of ventriculoperitoneal shunt is uncommon, but well-documented entity. The presentation may be without any symptoms or maybe with meningitis and peritonitis. In a patient with simple bowel perforation and no other complications, a formal laparotomy is not required, while presence of peritonitis will necessitate an urgent laparotomy. If detected in time and managed properly, dreaded complications can be prevented.
Acknowledgements
Acknowledgements are due to the Departments of Radiology and Imageology, Krishna Institute of Medical Sciences (KIMS), Secunderabad.
Conflicts of interest
Authors declare no conflicts of interest.
References
1. Acharya R, Ramachandran CS, Singh S. Laparoscopic management of abdominal complications in ventriculoperitoneal shunt surgery. J Laparoendosc Adv Surg Tech A. 2001; 11(3):167–170.
2. Ferreira PR, Bizzi JJ, Amantea SL. Protrusion of ventriculoperitoneal shunt catheter through the anal orifice. A rare abdominal complication. J Pediatr Surg. 2005; 40(9):1509–1510.
3. Kanojia R, Sinha SK, Rawat J, Wakhlu A, Kureel S, et al. Unusual ventriculoperitoneal shunt extrusion: experience with 5 cases and review of the literature. Pediatr Neurosurg. 2008; 44(1):49–51.
4. Hai A, Rab AZ, Ghani I, Huda MF, Quadir AQ. Perforation into gut by ventriculoperitoneal shunts: A report of two cases and review of the literature. J Indian Assoc Pediatr Surg. 2011; 16(1):31–33.
5. Sarkar D, Sarkar S. Ventriculoperitoneal shunt catheter migration through umbilicus - a rare complication. Pediatric Oncall. 2010; 7(3).
6. Low SW, Sein L, Yeo TT, Chou N. Migration of the abdominal catheter of a ventriculoperitoneal shunt into the mouth: a rare presentation. Malays J Med Sci. 2010; 17(3):64–67.
7. Dagtekin A, Karabag H, Avc E, Nayc A, Bagdatoglu C. A rare complication with ventriculoperitoneal shunt in pediatric cases. Ege Journal of Medicine. 2011; 50(1):65–68.
8. Vuyyuru S, Ravuri SR, Tandra VR, Panigrahi MK. Anal extrusion of ventriculoperitoneal shunt tube: Endoscopic removal. J Pediatr Neurosci. 2009; 4(2):124–126.
9. Ozturk H, Is M, Ozturk H, Kucuk A, Dosoglu M. Transanal protrusion of a ventriculoperitoneal shunt catheter. J Coll Physicians Surg Pak. 2012; 22(11):733–734