Full Text
Proximal femoral focal deficiency (PFFD) is a rare congenital disorder involving the bones of the hip. It involves deficient development of proximal femur and in some cases even the acetabulum. Genetically, it is associated with sonic hedge-hog gene (Limb Bud), and is a rare autosomal dominant type. Clinically, the child may present with a swelling in the involved hip, deformity of the thigh and shortening of the limb. It may be bilateral. Idiopathic coxa vara is included as a part of PFFD spectrum if the varus is associated with congenital femoral shortening at birth i.e. type 1.
The pathophysiology mainly rests in the defect of primary ossification centre-cartilage anlage. The associated manifestations may include fibular hemimelia, coxa vara, oligodactyly, absent patella and contracture of the knee.
Investigations
Ultrasonography may play a role in the fetus and in early infancy. The cartilaginous portion is well defined by ultrasonography. When once the ossific centre appears in the femoral head, plain radiography plays a major role. Based on plain radiography the classification is made by Aitken (Table 1). This is the simplest and most widely used, which is based on the anatomic relationship between the acetabulum and the proximal end of the femur and is classified into four as the following:
Radiographic findings
Table 1: Aitken classification.
|
Class
|
Femoral Head
|
Acetabulum
|
|
A
|
Present
|
Normal
|
|
B
|
Present
|
Mildly dysplastic
|
|
C
|
Absent
|
Severely dysplastic
|
|
D
|
Absent
|
Absent
|
Class A (Figure 1abc)
i) This is the least severe type where the femoral head is present and attached to the shaft by the femoral neck. ii) The femur is shortened (as in all types), and a coxa vara deformity is present. iii) A cartilaginous neck is not seen on early radiographs but later ossifies. iv) Occasionally, the cartilaginous connection between the neck and the shaft forms a sub trochanteric pseudoarthrosis.
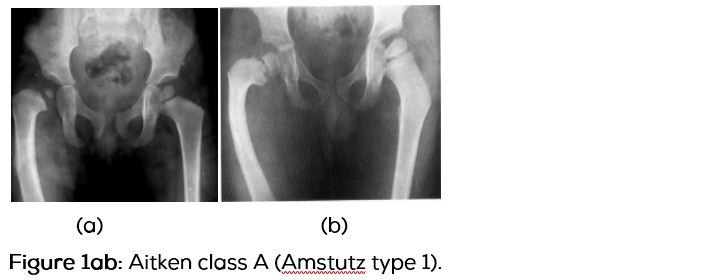
Results from an insult to the limb bud early in fetal life before the development of the hip joint has been completed. No familial tendency.

Class B (Figure 2ab)
i) In this type, the acetabulum is “adequate” or moderately dysplastic and contains the femoral head. ii) At maturity, no osseous connection is seen between the femoral head and the shaft. iii) The femoral segment is short and usually has a bulbous bony tuft.

Class C (Figure 3abc)
i) The acetabulum is severely dysplastic in this form. ii) The femoral head is absent or is very small and not attached to the femoral shaft. iii) The shortened femoral segment has a tapered proximal end. iv) Arthrogram shows the cartilaginous portion (Figure 3d)

Class D (Figure 4)
i) This is the most severe form, with absence of the acetabulum and proximal femur. ii) No proximal tuft is present.

Amstutz further subdivided Aitken’s classification into five types. He divided class A into types 1 and 2. Type 1 is reserved for the milder form with simple femoral shortening and coxa vara. In type 2, a subtrochanteric pseudoanthrosis is present. The remaining types correspond to those of Aitken’s classification.
Amstutz classifications
Five types: 1) Congenital short femur with bowing, coxa vara & normal acetabulum. 2) Short femur subtrochanteric pseudoarthrosis, progressive coxa vara & normal acetabulum. 3) Short femur with bulbous proximal end delayed appearance of capital epiphysis. Mild dysplastic acetabulum. 4) Short femur segment tapering sharply to a point at the proximal end acetabulum becomes progressively dysplastic. 5) Small bone segment representing the distal femoral shaft with no evidence of proximal femoral components & no acetabulum. Ipsilateral fibular hemimelia.
Several other classifications were proposed, but Aitken’s and Amstutz’s classifications
are the most widely used.
Since the management of type 1 varies from that of type 2, a distinction between them is necessary.
Role of computed tomography (CT)
In infants and children, CT should be rarely used following ALARA principle. However, for the surgeon 3D format of CT is quite helpful.
Role of magnetic resonance imaging (MRI)
Since, there is no exposure to ionising radiation and because of the multiformat images, this investigation is being preferred in recent times. The coronal and axillary images may be adequate. However, MR arthrography gives additional value.
MR imaging findings (Figure 5abc)
Determines the presence or absence of cartilaginous portion of the head of the femur and the presence of a connection between the head and shaft.

Differential diagnosis includes Idiopathic coxa vara of childhood which is of two types. One, congenital form-generally present at birth. Two, infantile form-not present at birth, recognised at around 4 years of age, and is often bilateral (33%). Occasionally, acetabular dysplasia with congenital dislocation of hip may be confused with PFFD (Figure 6). In neglected pyogenic arthritis of the hip, the sequalae may be likely to be mistaken for PFFD (Figure 7).

Radiographic findings of idiopathic coxa vara include bilaterality, vertically inclined epiphyseal plate, head low in acetabulum, outline of head may appear woolly, secondary deformity of acetabulum, triangular bone fragment at lower part of femoral neck and curved greater trochanter articulating with ilium (Figure 8).

Treatment is primarily surgical, which includes equalising limb length, correcting rotational anamolies, improving stability of hip joint and with marked shortening--prosthesis
Conclusion
Proximal femoral focal deficiency (PFFD) is a rare congenital disorder affecting the hip bones. A spectrum of imaging findings ranges from mild femoral shortening with various deformities to complete absence of both the acetabulum and proximal end of femur. Both Aitken’s and Amstutz classifications are described. Conventional radiography is the main investigation. However, MRI helps in determining the presence or absence of cartilaginous portion as the management differs.
Conflict of Interest
The author declares no conflict of interest.
References
1. Aitken GT. Proximal femoral focal deficiency: definition, classification, and management. Paper presented at a symposium on proximal femoral focal deficiency, Washington, D.C., June 1968, Washington, D.C., National Academy of Sciences. 1969; 1–22.
2. Amstutz HC, Wilson PD. Dysgenesis of the proximal femur (coxa vara) and its surgical management. J Bone Joint Surg Am. 1962; 44-A:1–24.
3. Finby N, Jacobson HG, Poppel MH. Idiopathic coxa vara in childhood. Radiology. 1956; 67(1): 10–16.
4. Gabriel H, Fitzgerald SW, Myers MT, Donaldson JS, Poznanski AK.. MR imaging of hip disorders. Radiographics. 1994; 14(4):763–781.
5. Maldjian C, Patel TY, Klein RM, Smith RC. Efficacy of MRI in classifying proximal focal femoral deficiency. Skeletal Radiol. 2007; 36(3):215–220.
6. Yochum TR, Rowe LJ. Essentials of Skeletal Radiology. Philadelphia, PA: Lippincott Williams & Wilkins, c2005. 2004; ISBN:078173946.