Full Text
Introduction
The prevalence of tumors of the ribs ranges from 3 to 8% depending on the series [1]. Tumor like lesions are more in number than primary tumors of the ribs [2]. Benign and primary malignant tumors of the ribs are rare and may be identified during the investigation of a clinically suspected abnormality or as an incidental finding [3]. This review describes the spectrum of benign and malignant tumors that can involve the rib and illustrates the radiographic, computed tomography (CT) and magnetic resonance (MR) imaging appearances that may facilitate diagnosis. The differential diagnosis of benign bone tumors of the ribs is also discussed with illustrations.
Imaging findings and discussion
Benign tumors include tumors arising from the following tissues [4]:
• Osseous tissue – Osteoid osteoma, osteoblastoma
• Fibrous tissue – Non ossifying fibroma
• Cartilaginous tissue – Enchondroma, exostosis, chondroblastoma, chondromyxoid fibroma
• Vascular tissue – Hemangioma
• Miscellaneous – Aneurysmal bone cyst (ABC), Giant cell tumor (GCT)
Benign Bone-forming tumors Osteoid osteoma is a localized bone forming tumor with a radiolucent nidus less than 1.5 cm diameter. It is rarely encountered in rib [5].
Osteoblastoma is a rare benign bone forming tumor. The nidus is larger than is seen in osteoid osteoma, generally more than 2 cm. It is well circumscribed and sometimes aggressive resembling osteosarcoma. The rib is a rare location (Figure 1) [6, 7].

Figure 1: Osteoblastoma rib, note the radiolucent nidus.
Tumors of cartilaginous origin
Benign tumor of cartilage (Enchondroma) arising from rib is relatively common. It generally arises from costochondral junction. The radiological findings of enchondroma include a lucent lobulated well-demarcated lesion with calcifications which are shaped arc like, circular, nodular and punctate (Figure 2a-c). There is no cortical break unless there is a history of trauma. When the lesion is large and with the presence of a pathological fracture, it is difficult to differentiate it from low grade chondrosarcoma [8]. CT demonstrates the typical cartilaginous calcifications and presence of soft tissue swelling when present (Figure 2d).
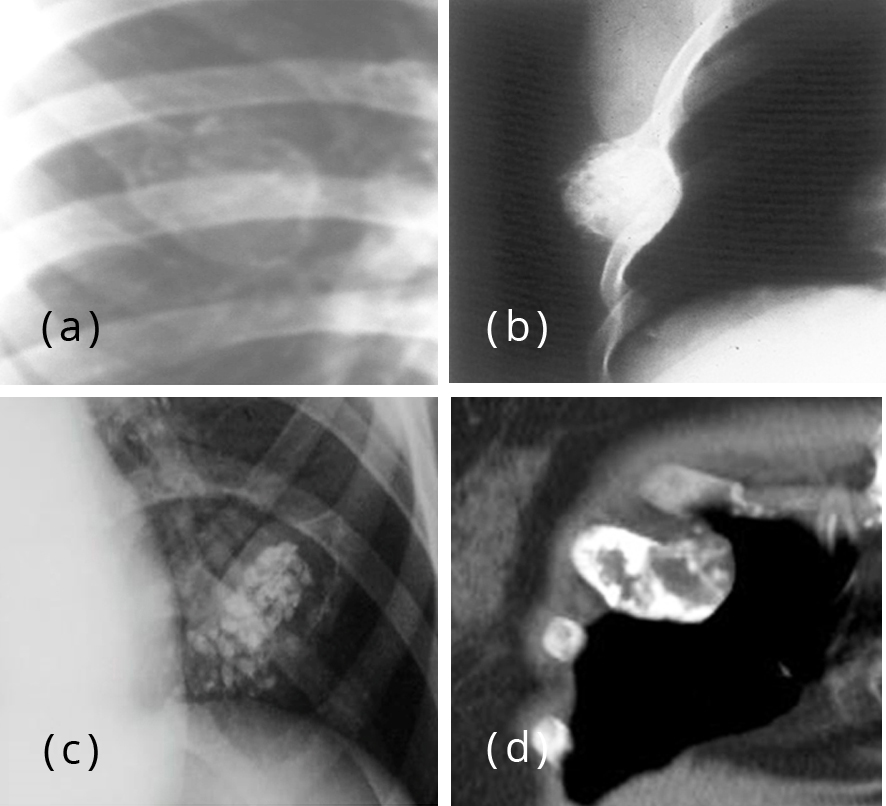
Figure 2: (a) Enchondromaof the rib, (b) Enchondroma rib with calcifications, (c) Enchondroma rib with nodular calcifications, (d) Enchondroma – CT.
Another cartilaginous lesion that arises from the rib is osteochondroma. It may be monostotic or polyostotic. When it is polyostotic, it is generalized (Figure 3a,b) and is hereditary. Radiologically there may or may not be a pedicle. It could be sessile. Osteochondroma grows outside the rib with a cartilaginous cap. Cartilage cap thickness is an important indicator of osteochondroma-to-sarcoma transformation. If it exceeds 2 cm in adults or 3 cm in children, malignant transformation should be suspected. Calcifications are often seen which are better demonstrated on CT (Figure 3c-e) [9].
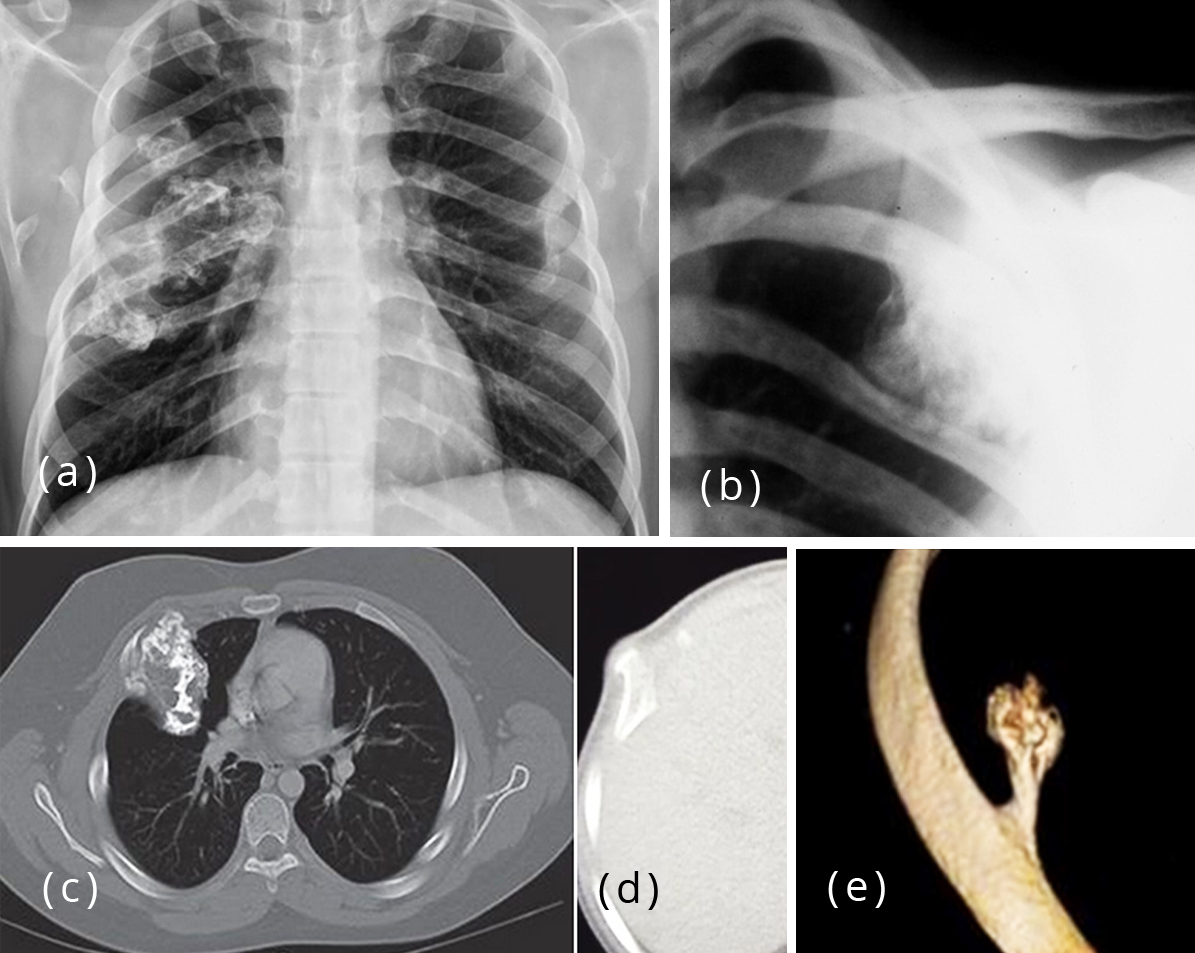
Figure 3: (a) Multiple exostoses of the ribs, (b) Exostosis of rib. Figure 3c,d: CT - Exostosis of the rib, (c) grows inside, (d) projects outside, (e) 3D CT - Osteochondroma rib with a pedicle.
Tumors arising from the vascular tissue
Hemangioma is one of the common benign tumors arising in the bone. However, hemangioma of the rib is relatively uncommon. It is well circumscribed with a “spoke wheel” pattern of trabecular distribution (Figure 4a). The trabeculae are thickened and may run in a parallel way [10, 11]. There may be sunray spicules appearance when seen “end on” (Figure 4b,c).
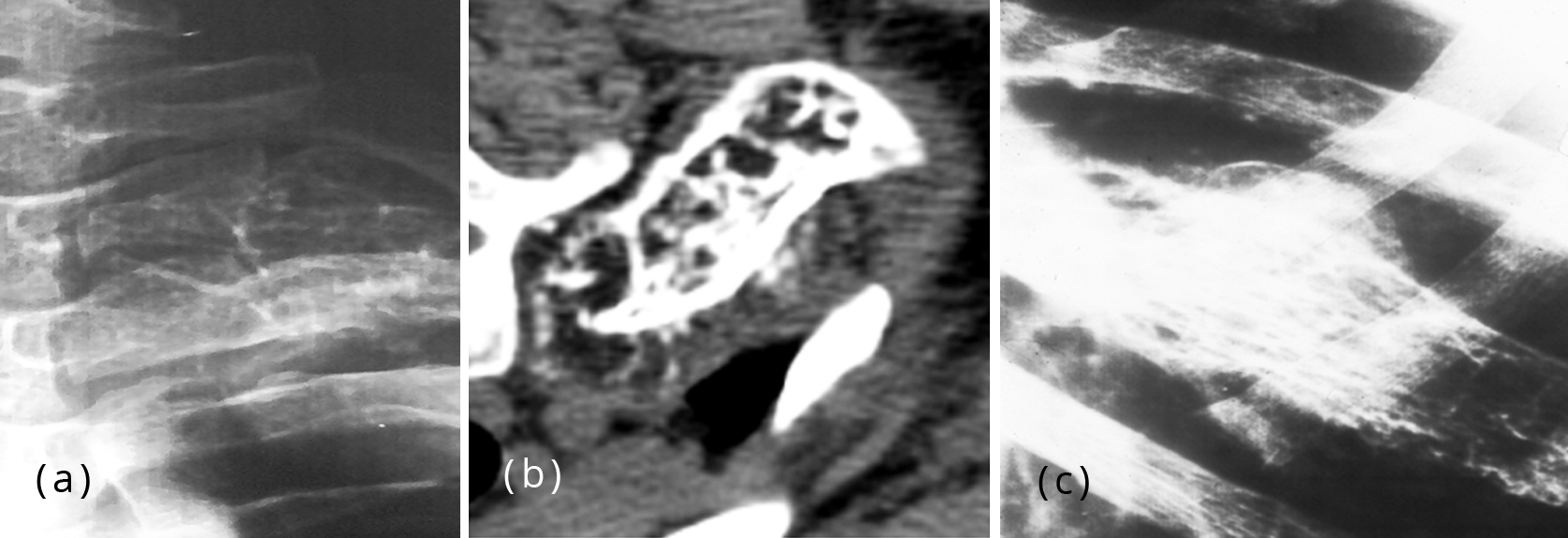
Figure 4: (a) Hemangioma with spoke wheel pattern, (b) Hemangioma thickened trabeculae, (c) Hemangioma of the rib with thickened parallel trabeculae.
Tumors arising from miscellaneous tissues
Aneurysmal bone cyst (ABC) can be primary or secondary. Radiologically, a well-defined large lytic area with a shell and a septated mass with a thin well defined rim are noted [12] (Figure 5a,b). On cross sectional imaging fluid-fluid levels may be seen (Figure 5c).
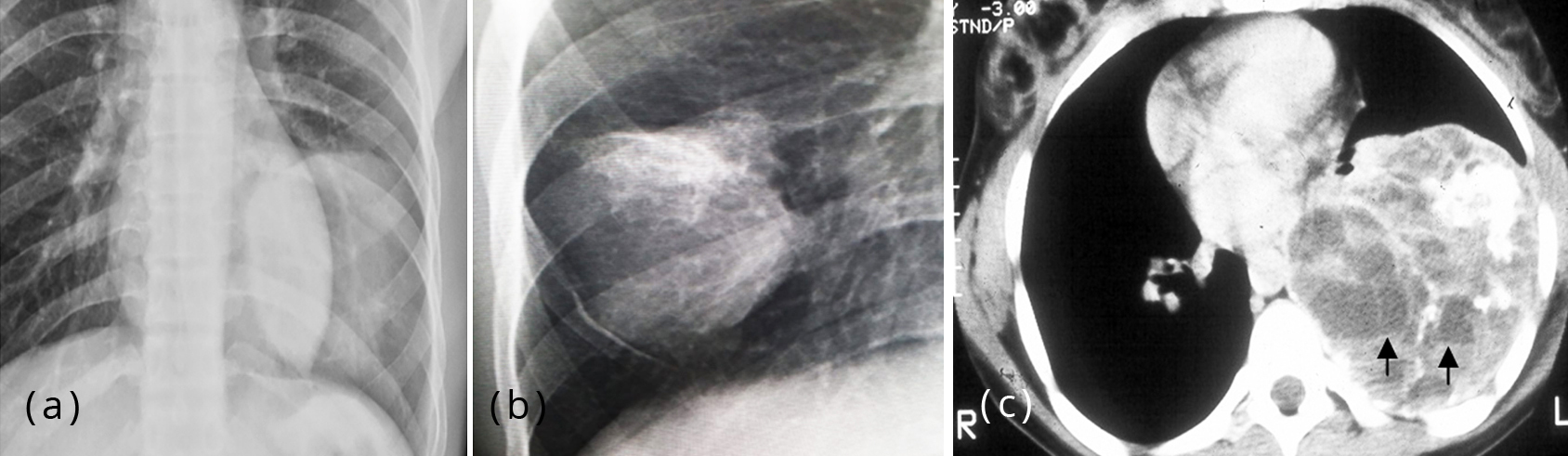
Figure 5: (a, b) Large ABC of the rib, (c) ABC CT with fluid-fluid levels.
Giant cell tumor (GCT) as compared with long bones is rarer in ribs. It is a large expanding lytic area with thick trabeculations simulating a soap bubble. No reactive new bone is noted [13]. It may be associated with secondary aneurysmal bone cyst (Figure 6).
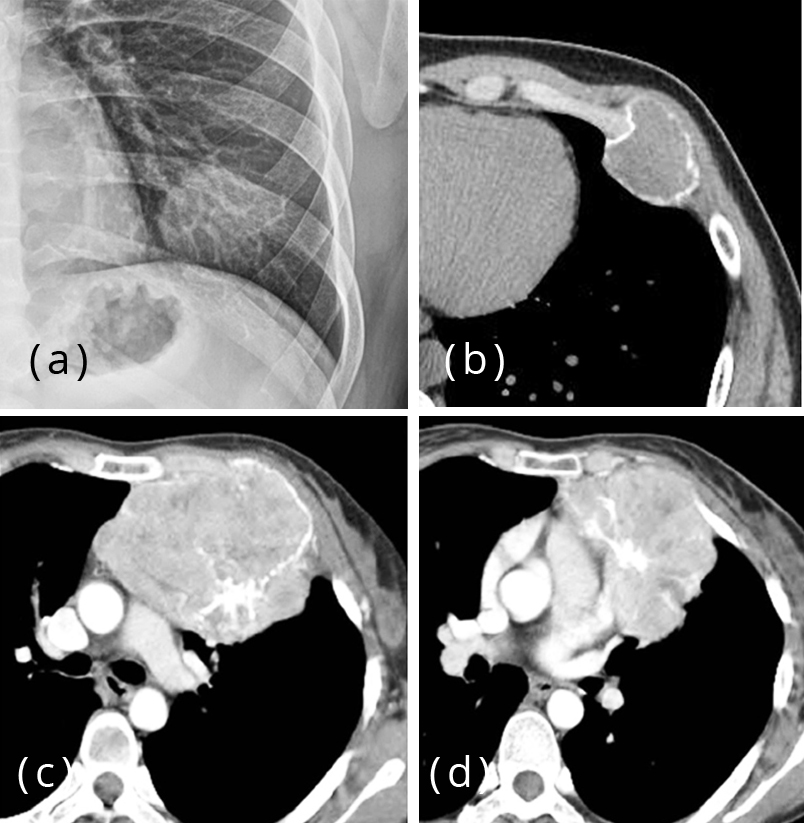
Figure 6: (a) Giant cell tumor (GCT) of rib, conventional radiology, (b-d) Giant cell tumor of rib – CT.
Primary malignant tumors of the ribs
The most common primary malignant lesions arising from the ribs include:
1. Chondrosarcoma
2. Plasmacytoma
3. Ewing’s and Ewing’s family of tumors
4. Osteosarcoma
5. Lymphoma
6. Hemangioendothelioma
Radiological characteristics of a malignant bone tumor consist of extensive cortical destruction and extraosseous soft-tissue mass formation. Mineralization is present in chondrosarcoma, Ewing’s and osteosarcoma.
Chondrosarcoma can be primary or secondary. Primary chondrosarcoma arises de novo (Figure 7a-f) whereas secondary chondrosarcoma arises generally from enchondroma or osteochondroma [14]. Radiologically, a very prominent soft tissue mass is noted with characteristic cartilaginous type of calcifications which may be in the shape of arcs, circles, punctuate or nodules [15] (Figure 7g,h). Cross sectional imaging is essential for diagnosis and management of the lesion.
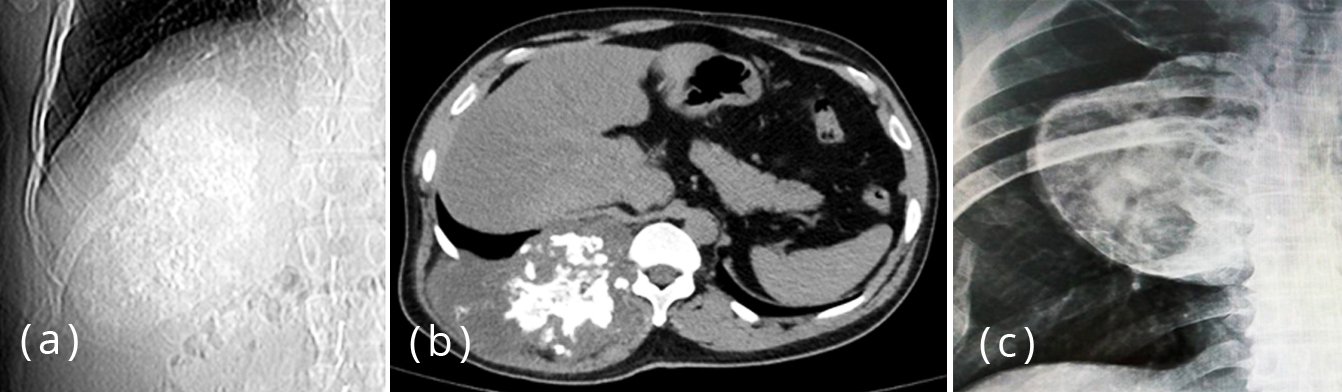
Figure 7a-c: (a, b) Chondrosarcoma of rib with calcifications, (c) Low grade chondrosarcoma with a well-defined margin.
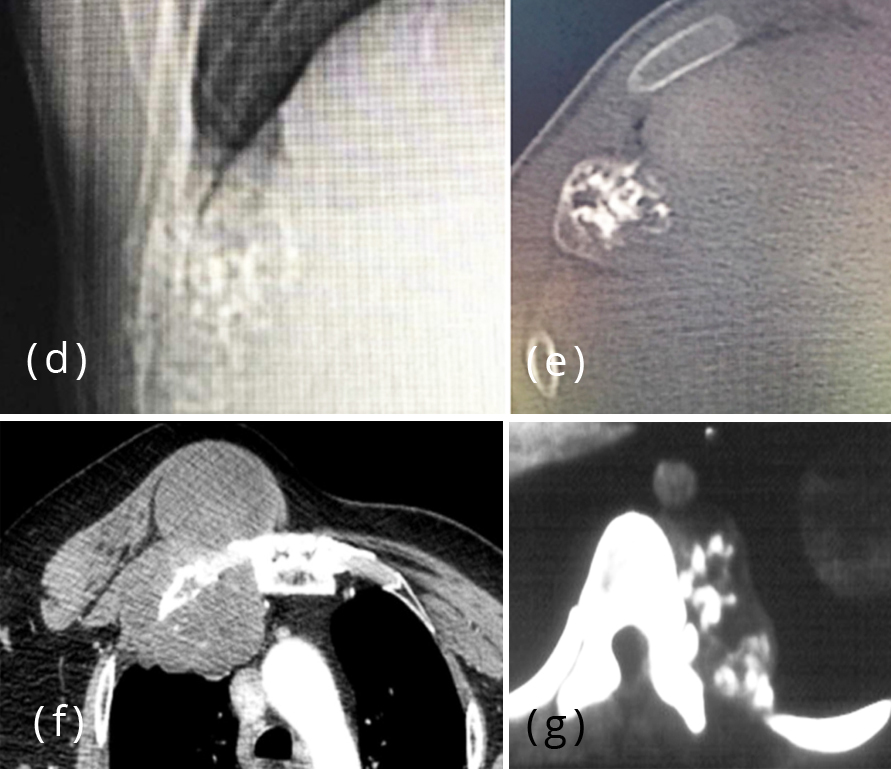
Figure 7d-g: (d, e) Low grade chondrosarcoma with scattered calcifications, (f) Primary chondrosarcoma with a large soft tissue mass, (g) Primary chondrosarcoma with nodular calcifications.

Figure 7h: Large osteochondroma with malignant changes.
Plasmacytoma is a localized form of multiple myeloma. It is noted that when solitary Plasmacytoma is followed, it may develop into multiple myeloma in 5-10 years [16]. Generally it occurs in older people with presentation of a soft tissue mass. Radiologically a lytic expansile lesion is noted with a soft tissue swelling. No reactive bone or periosteal reaction is noted unless there is a pathological fracture (Figure 8a,b) [17]. CT demonstrates the soft tissue swelling in a much better way (Figure 8c,d). Often it is difficult to differentiate from solitary lytic metastasis.
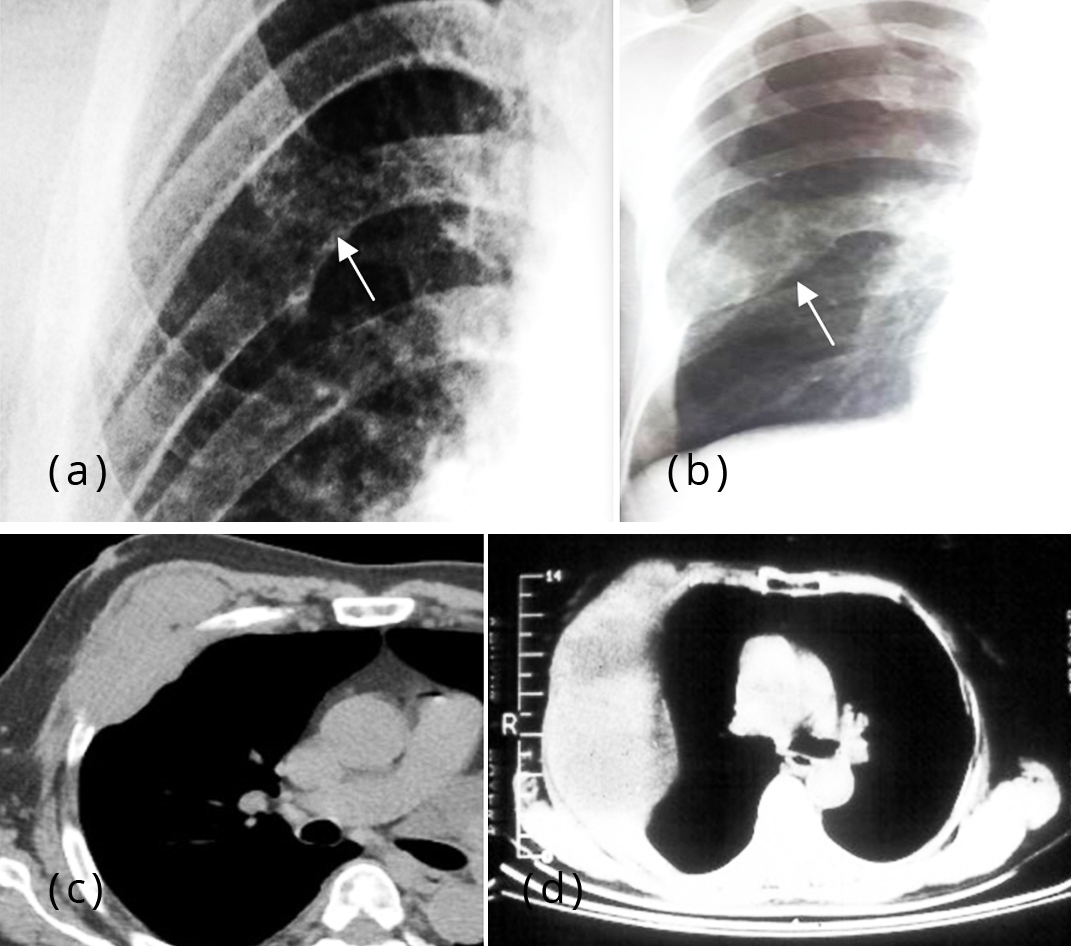
Figure 8: (a, b) Plasmacytoma of rib with a lytic lesion, (c, d) CT - Plasmacytoma of rib associated with a large soft tissue swelling.
Ewing’s sarcoma is a malignant tumor of bone of unknown origin. It is the second most common malignant tumor in children following osteosarcoma [18]. Ewing’s sarcoma includes a family of tumors:
– Ewing’s sarcoma (Bone –87%)
– Extraosseous Ewing’s sarcoma (8%)
– Peripheral PNET (5%)
– Askin’s tumor
Radiologically a moth eaten appearance of bone is noted with wide transitional zone (Figure 9a). It generally arises from the diaphysis and classically presents with an onion peel type of periosteal reaction. In the rib, soft tissue swelling is very prominent and generally it grows into the thorax rather than outside the chest wall [19] (Figure 9b-e). At times, it presents with great deal of reactive bone giving the appearance of an “Ivory” lesion (Figure 9f). One of the tumors from Ewing’s family of tumors is Askin tumor in which the rib involvement may be present [20] (Figure 9g,h).
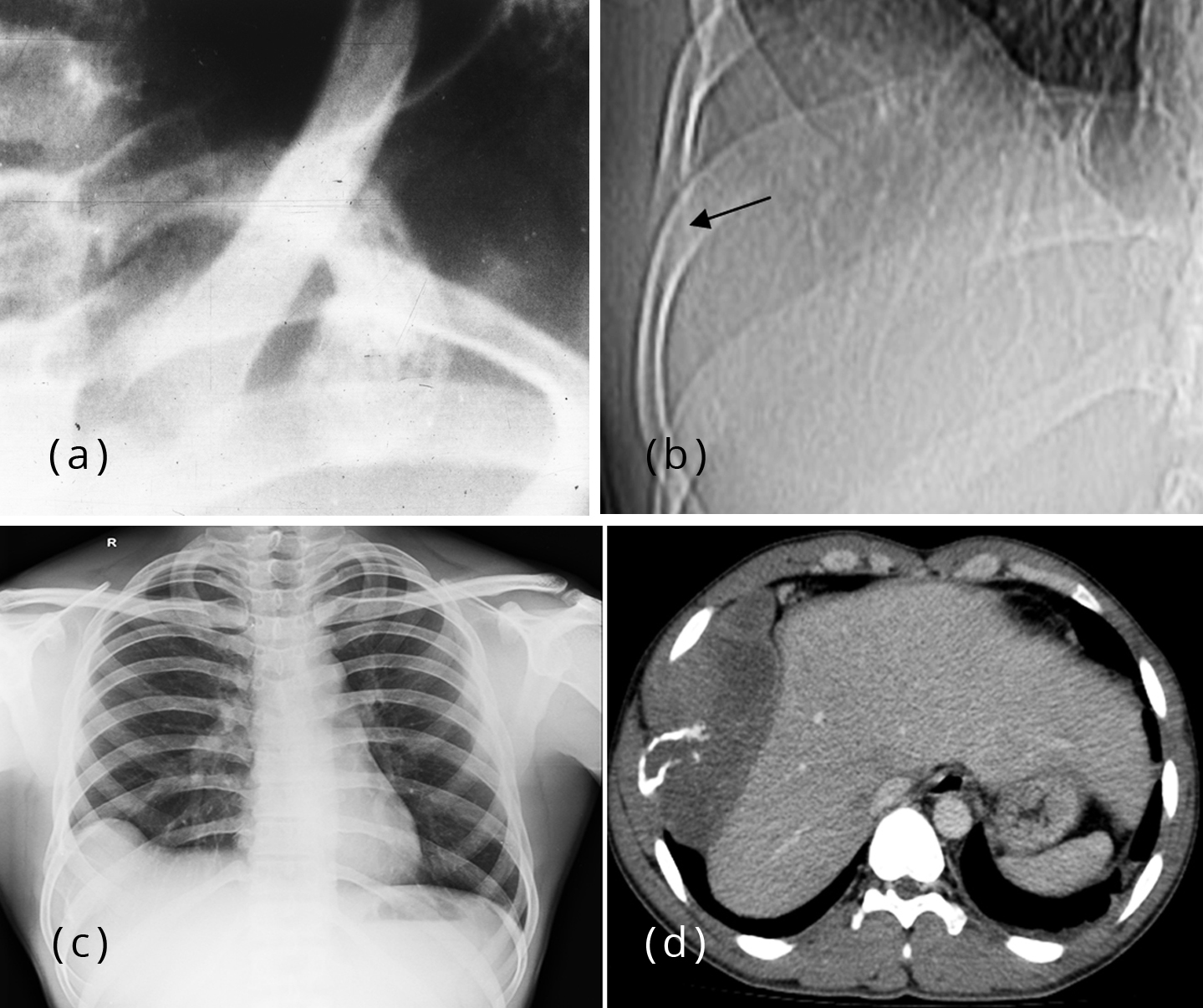
Figure 9a-d: (a) Ewing’s sarcoma rib with moth eaten appearance, (b) Ewing’s sarcoma with complete lysis of the rib, (c, d) Ewing’s sarcoma of the rib with soft tissue mass growing into the thoracic cavity.
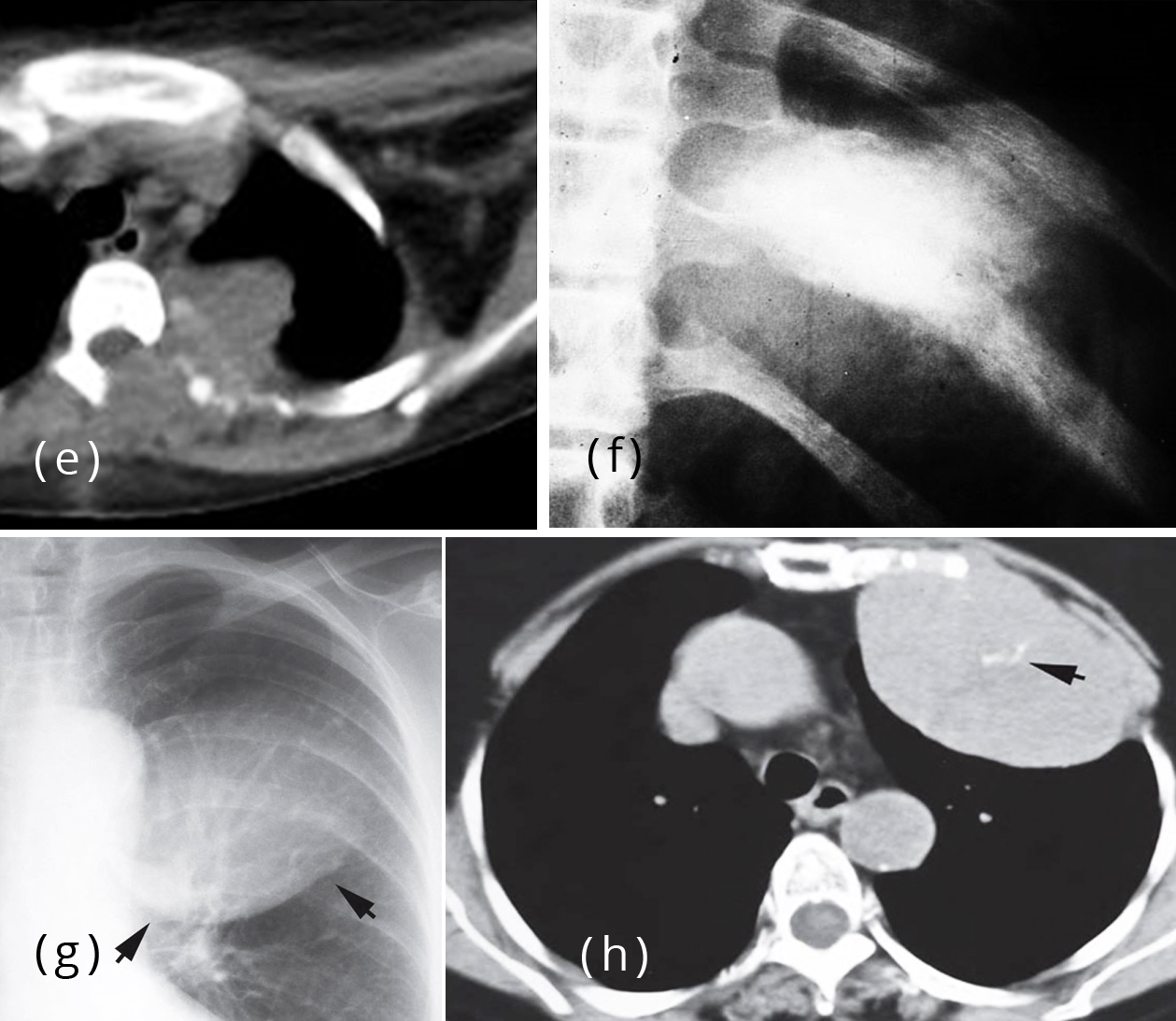
Figure 9e-h: (e) CT Ewing’s sarcoma extending into the vertebra, (f) Ewing’s sarcoma of rib with sclerotic new bone, (g, h) Askin tumor with a large soft tissue mass and erosion of the rib.
Osteosarcoma although is one of the common malignant tumors of long bones, in the rib it is not that common [21]. Radiologically, new bone formation in the form of osteoid clouds, periosteal reaction of various types and soft tissue mass are characteristic [22] (Figure 10). It may present with a pathological fracture. Cross sectional imaging helps in the diagnosis and management. MRI plays a great role in the study of soft tissues, vessels and nerves.
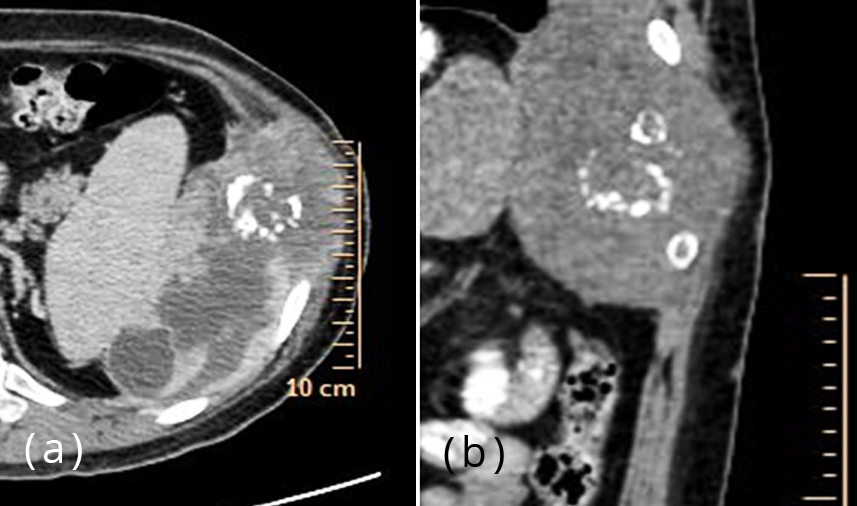
Figure 10a,b: Osteosarcoma of the rib, CT showing calcification and necrotic areas.
Primary lymphoma of the rib is extremely rare [23]. Radiologically it presents with a soft tissue swelling and a lytic area (Figure 11). There are no special imaging characteristics.
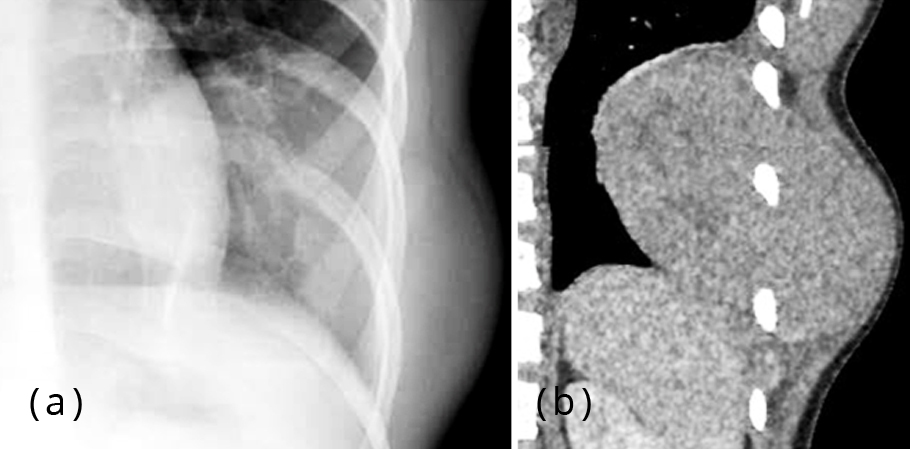
Figure 11a,b: Lymphoma of the rib with a soft tissue mass.
Hemangioendothelioma is a rare malignant vascular tumor of bones [24]. It is still rarer to encounter in the rib. Radiologically multiple lytic areas of various sizes are noted with no reactive or tumoral bone formation (Figure 12). Periosteal reaction is extremely rare. Soft tissue swelling is often present.
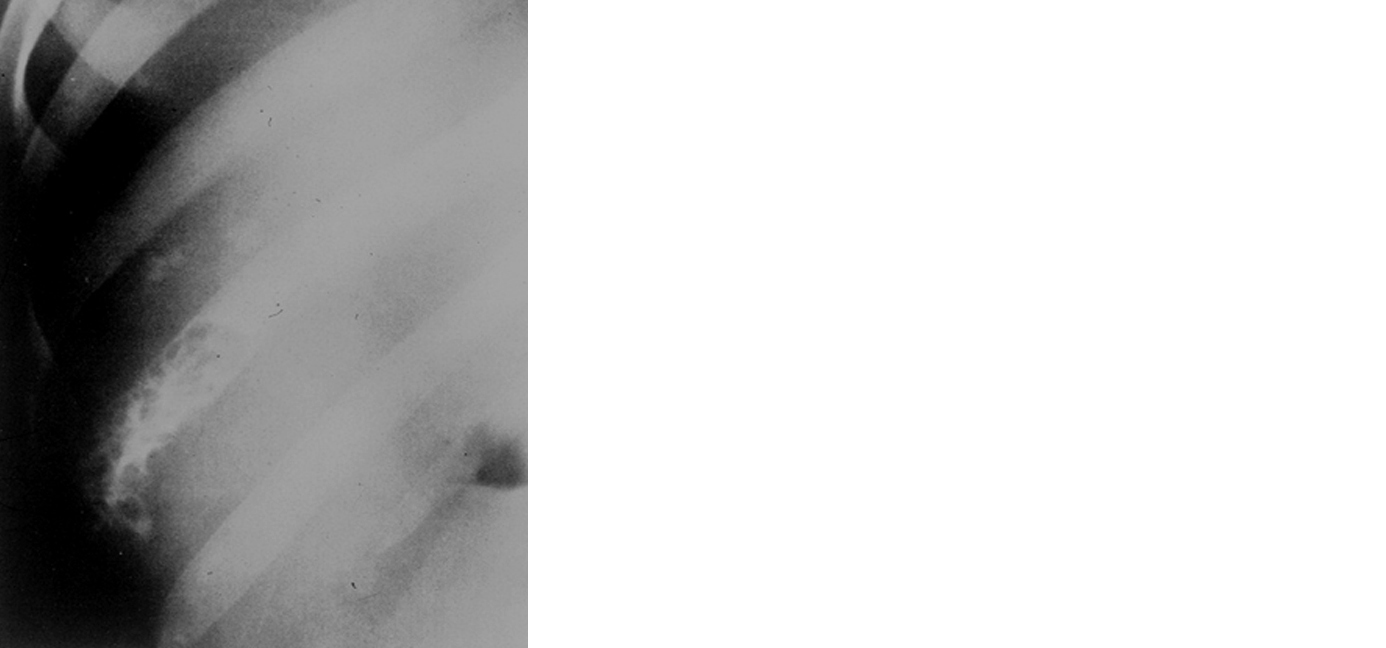
Figure 12: Hemangioendothelioma of the rib.
Differential diagnoses
Benign lesions simulating bone neoplasms
Tumor-like lesions of the ribs are occasionally encountered. These include congenital anomalies, infections, bacterial, parasitic, and fungal. Tumor-like lesions also include inflammations and other miscellaneous conditions.
Congenital anomaly
Bifurcation of the ribs is a common congenital anomaly either isolated or associated with some syndromes. The bifurcation of the rib should not be mistaken for pedenculated osteochondroma (Figure 13). In pedenculated osteochondroma, the base is small with a pedicle and a cartilaginous cap.
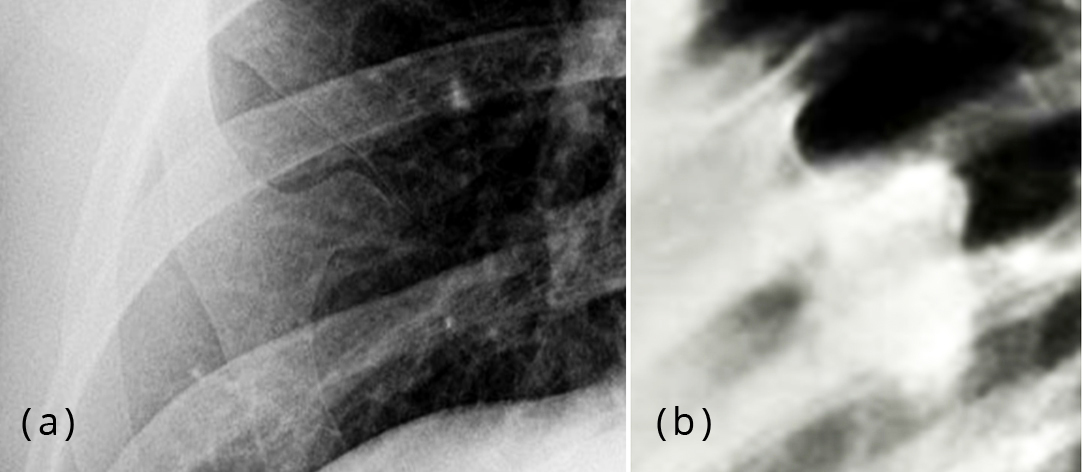
Figure 13: (a) Bifurcation of the rib, (b) Osteochondroma of the rib.
In the differential diagnosis of benign tumors, infection plays a major role which has an associated soft tissue swelling. Among these, tuberculosis is more common. Radiologically there is a lysis of the affected area with a soft tissue swelling. The characteristic feature of the soft tissue swelling is the central necrotic area indicating abscess [25]. This is best demonstrated on CT. In chronic cases, there may be calcification (Figure 14). Tuberculosis of the chest wall constitutes 1-5% of all cases of musculoskeletal tuberculosis. There is hematogenous seeding without active pulmonary disease.

Figure 14: Tuberculosis, (a) Lytic area, (b) CT cold abscess, (c) Lytic rib with soft tissue swelling.
Primary pyogenic infection of the rib is rare. There is osteolysis with irregular areas of lucency associated with periosteal reaction as seen in osteomyelitis of any other bone [26] (Figure 15).
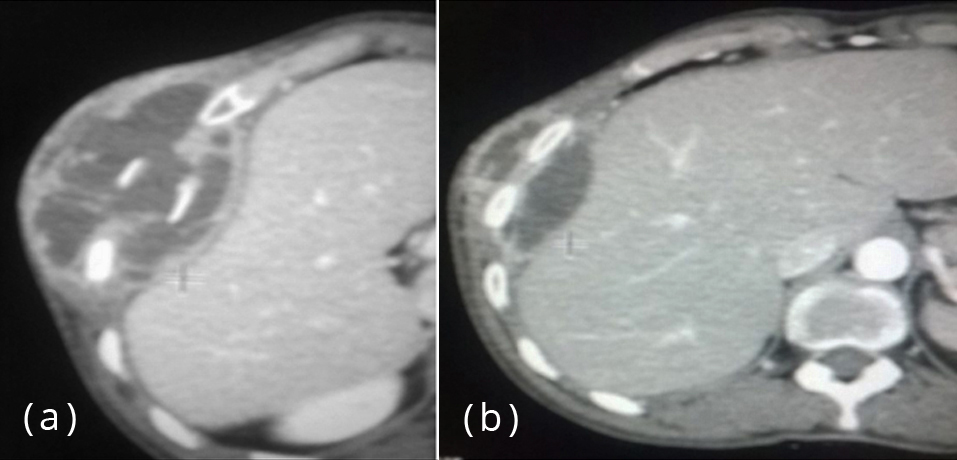
Figure 15a,b: Osteomyelitis of the rib with soft tissue swelling.
Fungal infections particularly actinomycosis Israeli may be occasionally encountered. The triad of characteristic features of actinomycosis involving of the rib includes pleura and lung parenchyma [27] (Figure 16). A sinus tract may be noted.
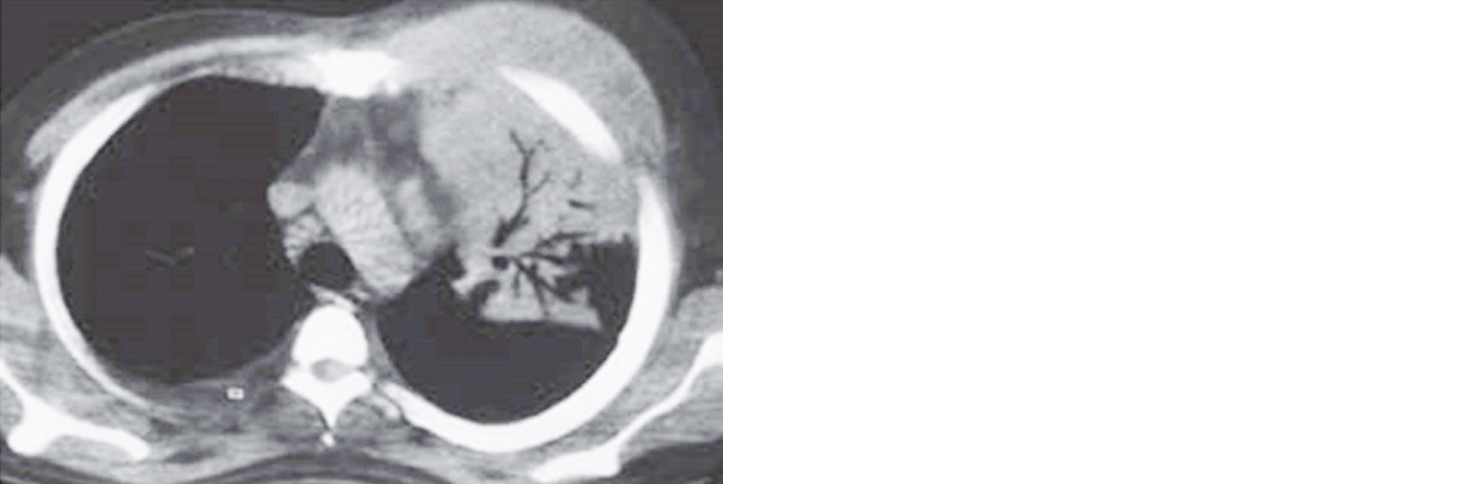
Figure 16: Actinomycosis involving the bone, soft tissues and lung parenchyma.
Parasitic infestation such as hydatid cyst may be encountered in the endemic area. A large expansile lesion with a lytic area is noted (Figure 17a). The lesion may be lobulated [28]. This is best demonstrated on CT (Figure 17b). Daughter cysts are also better demonstrated on CT.
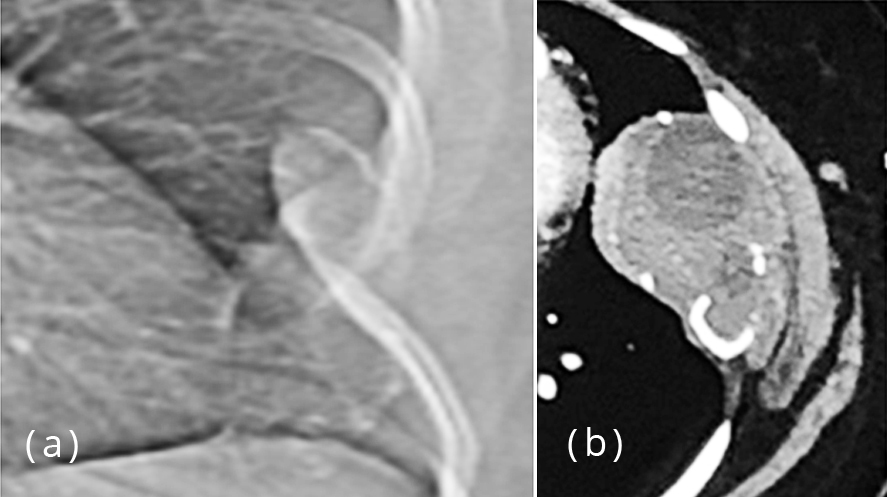
Figure 17: Hydatid rib, (a) Conventional, (b) CT showing daughter cysts.
Granulomatous lesions such as sarcoidosis and langerhans cell histiocytosis (LCH) may involve one or more ribs. Sarcoidosis of the ribs is extremely rare. LCH is relatively common and shows the same radiological features as seen elsewhere [29]. A lytic area with beveled edges with or without a soft tissue swelling is noted. Periosteal reaction is occasionally seen (Figure 18).
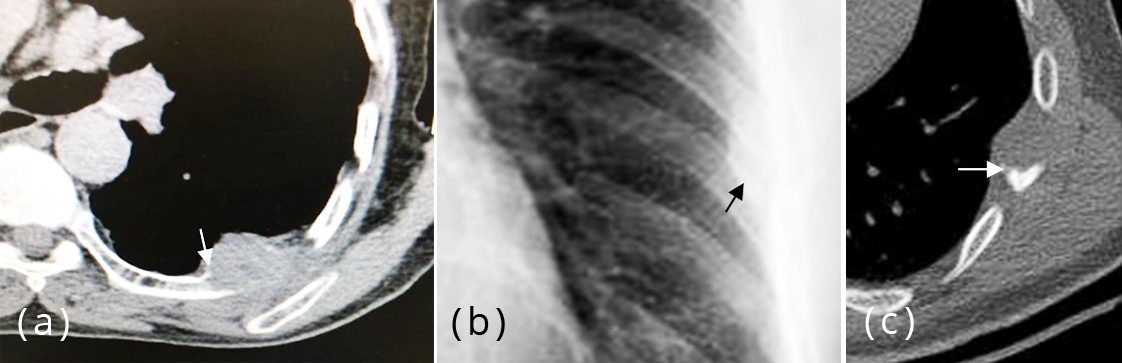
Figure 18a-c: LCH – lytic area with beveled edges and a soft tissue swelling.
Fibrous dysplasia (FD)
Fibrous dysplasia is a developmental aberration. Osteoblasts fail to form and are replaced by immature bone with fibrous stroma [30]. It is a common skeletal dysplastic lesion. It may be monostotic or polyostotic. Albright syndrome consists of polyostotic dysplastic lesions generally symmetrical, cutaneous pigmentation and endocrinal abnormalities. Mazabraud syndrome consists of fibrous dysplasia associated with soft tissue myxoma. Focal fibrous dysplasia of the rib shows a well outlined elongated lytic area with multiple lucencies and irregular reactive bone (Figure 19a). However, it may be purely sclerotic (Figure 19b) and a cystic type also has been described (Figure 19c). Ground glass appearance of the matrix is seen with rare presence of calcifications. It may be focal or diffuse involving the entire rib.
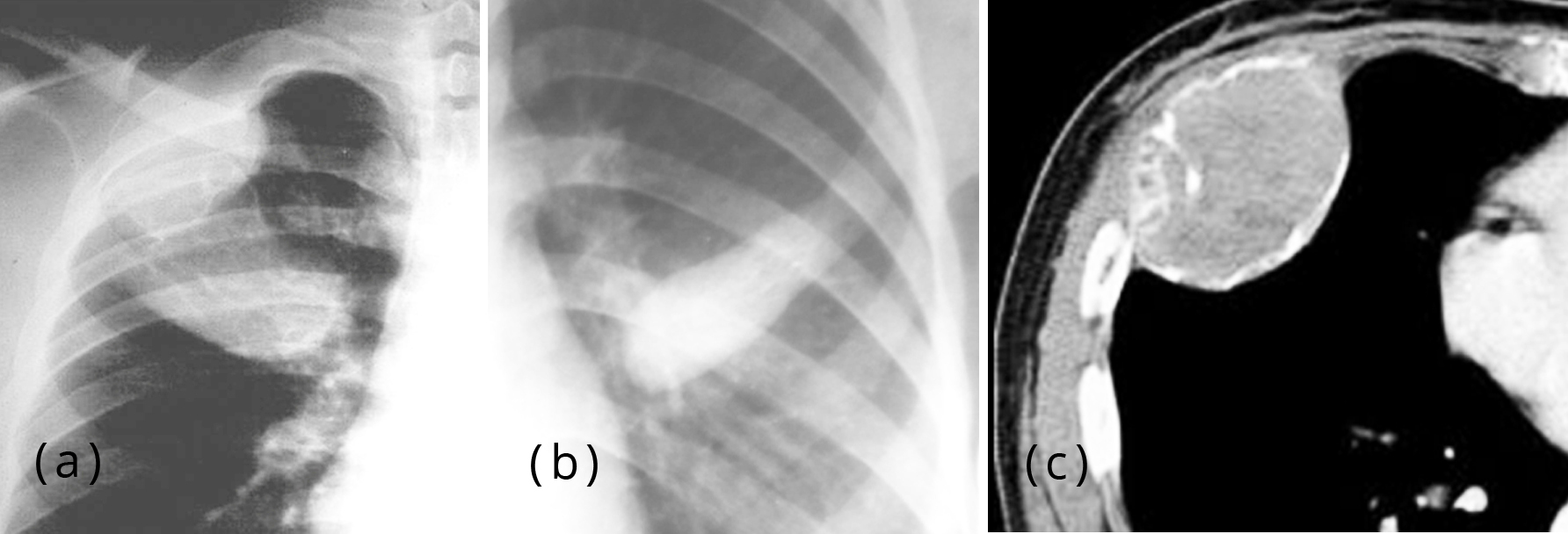
Figure 19: (a) FD – Expansile ground glass appearance of the 1st rib, (b): Monostotic FD – completely osteosclerotic, (c) FD – expansile lytic area with ground glass appearance.
Melorheostosis is a developmental skeletal dysplasia where the new bone flows along the longitudinal diameter of the bone (Figure 20). It gives a melting wax appearance. Generally it involves multiple bones and is rare in the ribs. It is purely a sclerotic area without periosteal reaction [31]. Soft tissue involvement may be noted.
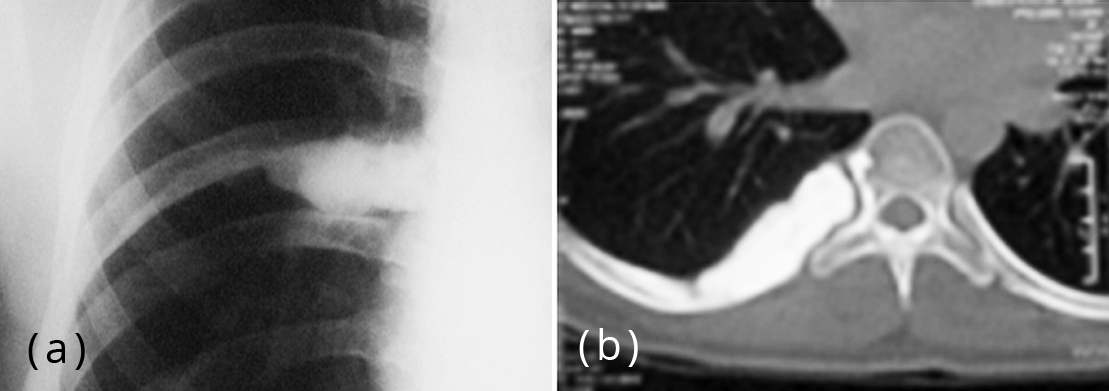
Figure 20a,b: Melorheostosis – flowing hyperostosis involving the vertebra and rib.
Conclusion
Primary tumors arising from the rib include benign and malignant. A number of benign tumors and their radiological characteristics are shown. Similarly included are primary malignant lesions of the rib. Differential diagnoses mainly for benign tumors are given including some rare entities. The illustrations mainly include conventional radiology but CT images are also added.
Acknowledgements
NIMS, KIMS, KREST Museum, Hyderabad, India.
Conflicts of interest
Author declares no conflicts of interest.
References
[1] Barrett NR. Primary tumors of rib. Br J Surg. 1955; 43:113–132.
[2] Sharma R, Gaillard F. Tumors of the chest wall (differentials). Available from: https://radiopaedia.org/articles/tumours-of-the-chest-wall-differentials
[3] Nam SJ, Kim S, Lim BJ, Yoon CS, Kim TH, et al. Imaging of primary chest wall tumors with radiologic-pathologic correlation. RadioGraphics. 2011; 31(3):749–770. Available from: https://doi.org/10.1148/rg.313105509
[4] Hughesa EK, Jamesa SLJ, Butta S, Daviesb AM, Saifuddina A. Benign primary tumours of the ribs. Clinical Radiology. 2006; 61(4):314–322.
[5] Deng Z, Ding I, Hao L, Yang F, Gong L, et al - Osteoid osteoma of the rib: A report of two cases. Oncol Lett. 2015; 9(4):1857–1860.
[6] Saber M, Weerakkody F. Osteoblastoma. Radiopaedia. Available from: https://radiopaedia.org/articles/osteoblastoma
[7] Katsenos S, Archondakis S, Sakellaridis T. Osteoblastoma of the rib: A rare benign tumor with an unusual location. Int J Surg Case Rep. 2013; 4(2):146–148.
[8] Jones J. Rib enchondroma. Radiopedia. Available from: https://radiopaedia.org/cases/rib-enchondroma-1
[9] Kadu VV, Saindane KA, Goghate N, Goghate N. Osteochondroma of the Rib: A rare radiological apeareance. J Orthop Case Rep. 2015; 5(1):62–64.
[10] Holland M. Rib hemangioma. Radiopedia. Available from: https://radiopaedia.org/cases/rib-haemangioma
[11] Park JY, Park JG, Lee SJ. Cavernous Hemangioma of the Rib: A case report. Iran J Radiol. 2016; 13(3):e31677.
[12] Yasaroglu M, Ketenci B, Demirbag H, Yildirim M, Dogusoy I. Aneurysmal bone cyst of the rib: A case report. J Med Cas Rep. 2009; 3:8457.
[13] Manjunatha HK, Ramaswamy AS, Kumar BS. Aggressive giant cell tumor of the anterior arc of the rib. Available from: http://www.jcytol.org/article.asp?issn=09709371;year=2012;volume=29;issue=1;spage=51;epage=53;aulast=Manjunatha
[14] Iqbal S, Bronson R. Chondrosarcoma. Radiopedia. Available from: https://radiopaedia.org/articles/chondrosarcoma
[15] Rascoe PA, Reznik SI, Smythe WR. Chondrosarcoma of the Thorax. Sarcoma. 2011:342879. Available from: https://www.hindawi.com/journals/sarcoma/2011/342879/
[16] Singal R, Dalal U, Dalal AK, Attri AK, Gupta S, et al. Solitary plasmacytoma of the rib: A rare case. Lung India. 2011; 28(4):309–311.
[17] Singh A, Patel R, Singh A, Patel RH, Devgarha S, et al. Solitary plasmacytoma of rib in a young adult – a rare case report. IOSR J Dent Med Sci. 2014; 13(9):56–59.
[18] Gilcrease-Garcia B. Ewing sarcoma – rib. Radiopedia. Available from: https://radiopaedia.org/cases/ewing-sarcoma-rib
[19] Paulussen M, Ahrens S, Dunst J, Winkelmann W, Exner GU, et al. Localized Ewing tumor of bone: Final results of the cooperative Ewing’s sarcoma study CESS 86. J Clin Oncol. 2001; 19(6):1818–1829.
[20] Keehn B, Jorgensen SA, Towbin AJ, Richard Towbin R. Askin tumor. Applied Radiology. 2017; Available from: https://appliedradiology.com/articles/askin-tumor [21] Ganguly S. Primary rib osteosarcoma: A rare entity. Available from: http://www.ccij-online.org/article.asp?issn=22780513;year=2015;volume=4;issue=3;spage=375;epage=377;aulast=Ganguly
[22] Abdulrahman RE, White CS, Templeton PA, Romney B, Moore EH, et al. Primary osteosarcoma of the ribs: CT findings - Skeletal Radiology. 1995; 24:127–129.
[23] Krishnan A, Shirkhoda A, Tehranzadeh J, Armin AR, Irwin R, et al. Primary Bone Lymphoma: Radiographic–MR Imaging Correlation. RadioGraphics. 2003; Available from: https://doi.org/10.1148/rg.236025056
[24] Mlika M, Ismail O, Marghli A, Boudaya S, Kilani T, et al. Epithelioid Hemangioendothelioma of the Rib: A Rare Tumour with a Confusing Localization. J Clin Exp Pathol. 2014, 4(2):159.
[25] Grover SB, Jain M, Dumeer S, Sirari N, Bansal M, et al. Chest wall tuberculosis - A clinical and imaging experience. Indian J Radiol Imaging. 2011; 21(1):28–33.
[26] Schubert R. Primary Osteomyelitis of the Chest Wall. Radiopedia. Available from: https://radiopaedia.org/cases/primary-osteomyelitis-of-the-chest-wall
[27] Han JY, Lee KN, Lee JK, Kim YH, Choi SJ, et al. An overview of thoracic Actinomycosis: CT features. Insights Imaging. 2013; 4(2):245–252.
[28] Roman A, Georgiu C, Nicolau D, Sabha W, Surariu M, et al. Cystic Hydatidosis of the Rib–Case Report and Review of the Literature - Ann Thorac Cardiovasc Surg. 2015; 21(5): 492–495.
[29] Kim SH, Choi MY. Langerhans Cell Histiocytosis of the Rib in Adult: A Case Report - Case Rep Oncol. 2016; 9(1):83–88.
[30] Kakarla S. Imaging in fibrous dysplasia. J Med Sci Res 2013; 1(2): 74–81. http://dx.doi.org/10.17727/JMSR.2013/1-014
[31] Semionov A, Jaffer R, Kosiuk J. Melorheostosis of a rib. Radiol Case Rep. 2018; 13(4):886–889.