Full Text
Introduction
Mesothelial cysts of the round ligament are developmental disorders. They are very rare and hard to diagnose. Most of them are asymptomatic or tend to produce abdominal pain, discomfort sensation of heaviness and abdominal distension. They are frequently misdiagnosed as ovarian cysts [11], irreducible inguinal hernias [1], femoral hernias [10], lipomas, peritoneal inclusion cyst, para ovarian cyst, mucocele of appendix, uterine leiomyoma, lymphocele, lymphangioleiomyomatosis, hematoma and abscess. Ultrasound and computerized tomography (CT) scan are the imaging modalities used for diagnosis but definitive diagnosis is usually made intraoperatively and confirmed histopathologically.
Case report
A 48-years-old female, two pregnancies and two children alive, presented to outpatient department with abdominal distension associated with discomfort since eight months. The patient had difficult to breath since two months and urinary incontinence since two months. No history of disturbances in bowel habits, vomitings or fever. Patient was married for 30 years, her last child birth was 18 years ago. Her vaginal deliveries were normal at private nursing homes. The patient never took oral contraceptive pills and she had not abdominal surgeries. Her menstrual cycles were regular and normal. There is no weight loss, loss of sleep and appetite. No personal or any personal family had any kind of illness.
On examination, the patient was moderately built and nourished. Respiratory and cardiovascular systems were normal. Per abdomen examination showed a cystic mass of 32-34 weeks gravid uterus size, mobile from side to side, all except lower border palpable, no tenderness, no palpable hepatosplenomegaly, and no free fluid noticed in the abdomen.
On per speculum examination, cervix and vagina were healthy but, on vaginal examination, uterus size could not be assessed. Bilateral forniceal fullness was present and non-tender.
Investigation
Ultrasound revealed a large cystic space occupying lesion in abdomen measuring 20×17×21cms size with thick septa, probably arising from right adnexa.
CT abdomen pelvis with contrast was advised. Report was suggestive of large cyst from right adnexa of size 19×16.4×20cms with enhancing hyper dense solid component within lesion abutting right distal ureter, anterior abdominal wall, bilateral common iliac vessels and displacing bowel loops, uterus and left adnexa normal ovarian tumour markers like CA125, CEA, Alfafetoprotein, CA 19-9 were within normal limits. Routine blood investigations were normal, except hemoglobin. It was 8.6 gm%.
Management
Patient was advised to undergo laparotomy and proceed. Transfusion of 1 unit of PRBC was done in view of low hemoglobin level of 8.6 gm% before surgery. MRI abdomen and pelvis was done to rule out malignant features of cyst such as solid components, metastasis involving other organs.
Intraoperative findings and procedure
The anaesthesia was under spinal and an usual laparotomy was made with sub umbilical midline incision. A large cyst was seen occupying whole abdominal cavity, cystostomy was done. Thick cyst wall noted, straw coloured fluid was aspirated, cystostomy opening was clamped and specimen was retrieved, cyst was seen arising from right broad ligament. Uterus was just bulky, bilateral tubes and ovaries were normal (Figure 1).
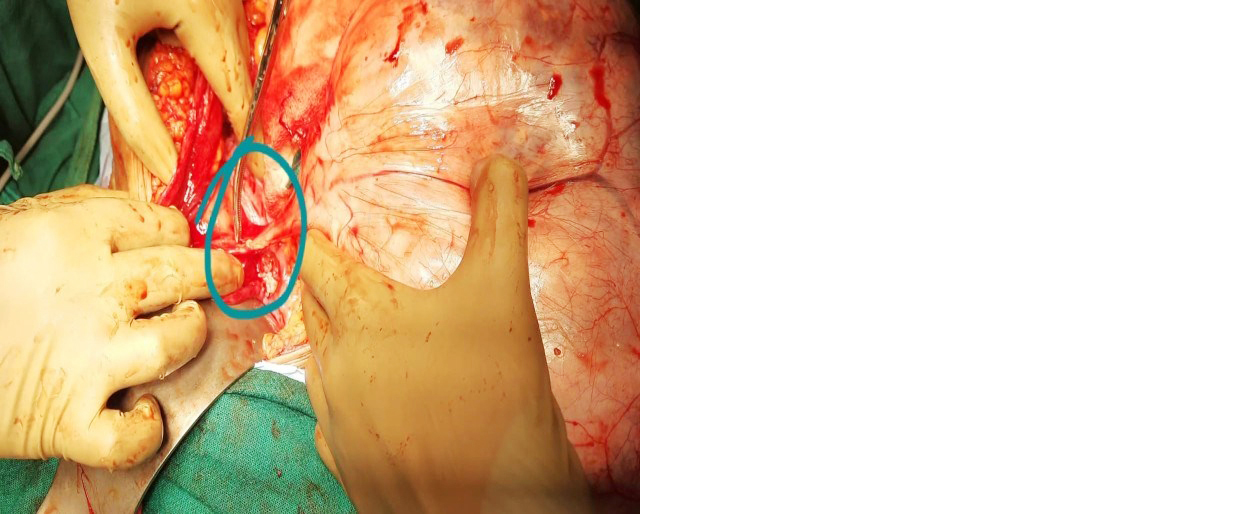
Figure 1: Showing cyst arising from right round ligament of uterus.
Decapsulation of cyst was done and dissection of broad ligament was done showing cyst arising from right round ligament (Figure 2), which was later clamped, cut and ligated and sent for histopathological examination. Mesothelial cyst with chronic inflammation lined by flattened cuboidal cells with characteristic appearance of mesothelial cells with smooth muscles, dense fibrous tissue and capillaries in the cyst wall (Figure 3).
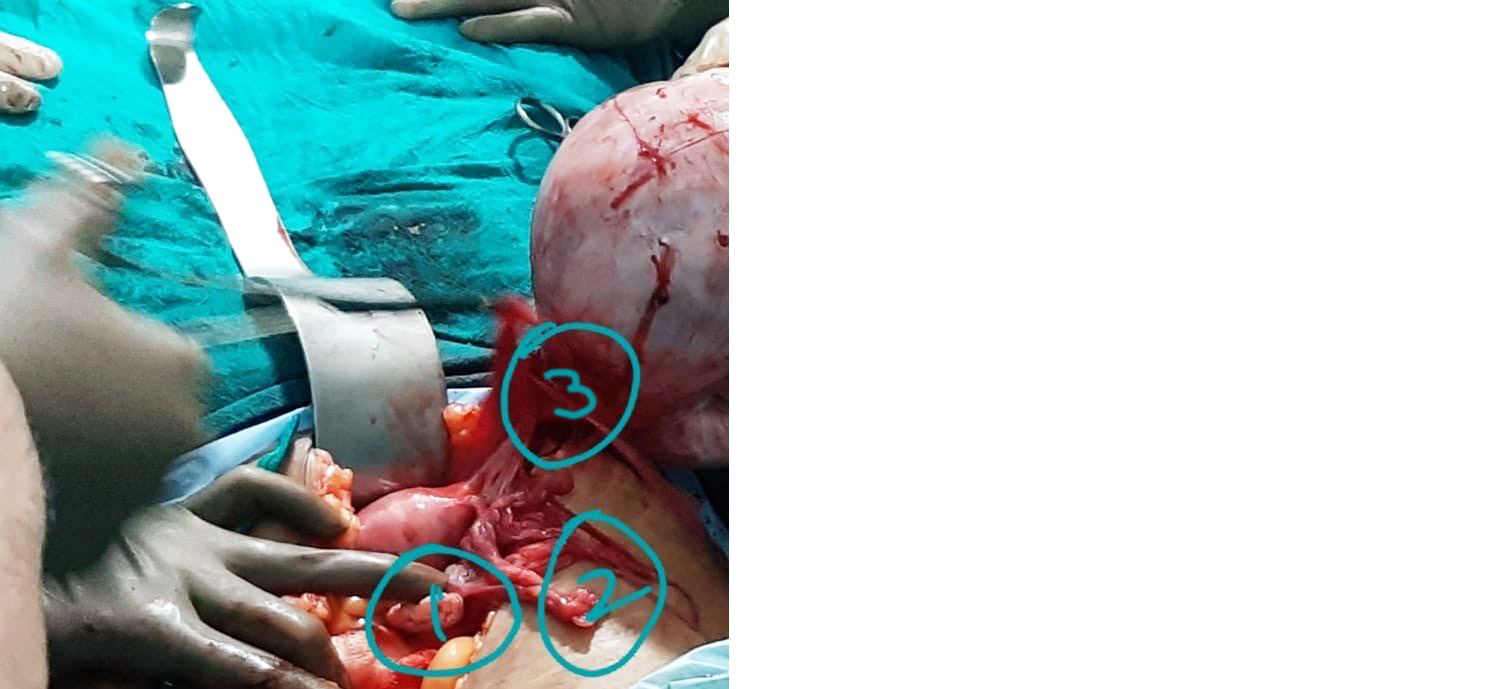
Figure 2: (1) Right ovary, (2) right Fallopian tube, (3) dissection of base of cyst showing it arising from right round ligament.
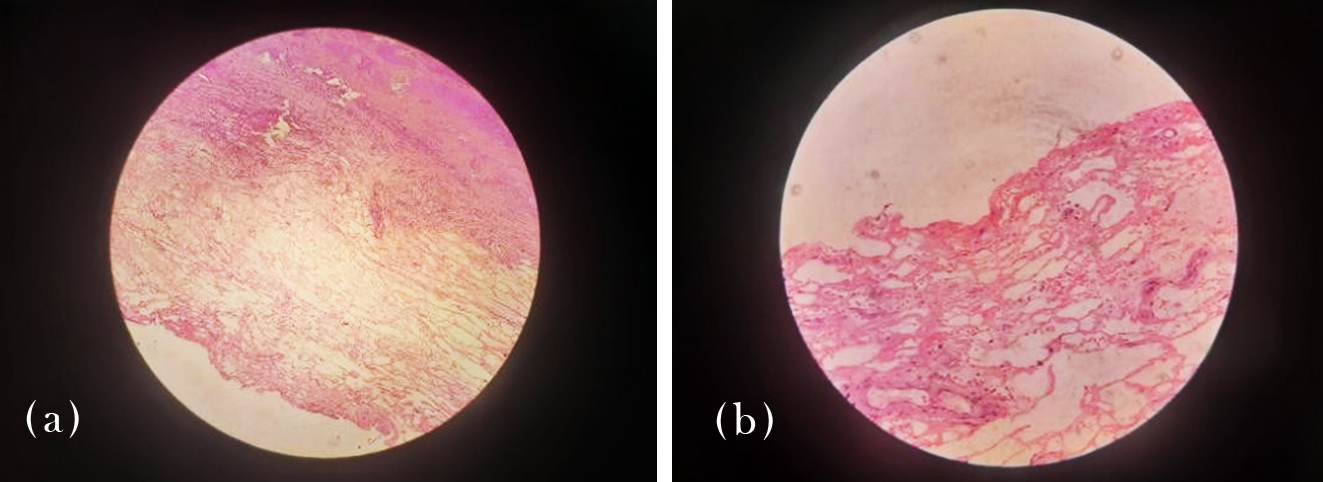
Figure 3a,b: Histopathology report was suggestive of mesothelial cyst arising from round ligament, lined by flattened cuboidal cells with characteristic appearance of mesothelial cells resting on an edematous fibromuscular and collagenous wall with a few thick walled vessels.
The post-operative period happened without problems. The patient has recovered and after second post-operative day and was discharged in good conditions. There was no report of recurrence.
Discussion
The round ligament of uterus extends from the uterus, passes through inguinal canal and ends in mons pubis in females. Embryologically, this is female counterpart of gubernaculum of testis and is predominantly composed of smooth muscle fibre, connective tissue, blood vessels and nerves with a mesothelial coating [2].
Two possible theories to explain the origin of round ligament cyst i.e., (i) Failure to obliterate of Nuck’s canal, (ii) Inclusion of embryonic mesenchymal elements or remnants the development of the round ligament [1].
Given the benign nature of the disorder, if the cyst is small it is possible to observe the asymptomatic patient with serial ultrasound. If the cyst becomes symptomatic or grow is better to make surgery [4]. Following excision prognosis is excellent and no recurrence is noted.
Mantakis et al [1] reported about a case which presented as irreducible inguinal mass which was later diagnosed intra operatively as round ligament cyst and confirmed by histopathology. As in our case, misdiagnosis is often common and is only confirmed intra operatively and histopathological evidence.
Choi, Lee YW published two case reports and literature review. A mesothelial cyst presenting as inguinal mass and the first diagnose was lymphangioma, but only intra operative was possible to find the real diagnose and it was confirmed as mesothelial cyst by histopathology and immunohistochemical staining.
Vargas-Ávila et al [8] described about a case which presented as incarcerated inguinal hernia in a 19-years-old girl with severe pain abdomen. Intra operatively it was found to be round ligament cyst and histopathologically confirmed as mesothelial cyst.
As in the above case reports, usually it presents as an inguinal mass, often misdiagnosed whereas in our case, it presented as large abdominal mass diagnosed as adnexal mass pre operatively, which later on was diagnosed intra operatively as round ligament cyst.
Conclusion
Although rare, a mesothelial cyst of intraperitoneal round ligament should be included in the differential diagnosis of inguinal mass or adnexal mass in female patients. Differential diagnosis is clinically difficult. Computerised tomography scan or an ultrasound scan would be a useful tool in diagnosis. Ovarian tumour markers should be done to rule out ovarian malignancy. The definitive diagnosis is made intraoperatively until confirmed histopathology.
Conflicts of interest
Authors declare no conflicts of interest.
References
[1] Manatakis DK, Stamos N, Agaliamos C, Vamvakas P, Kordelas A, et al. Mesothelial cyst of the round ligament misdiagnosed as irreducible inguinal hernia. Case Rep Surg. 2013; 2013:408078.
[2] Choi, Woon K, Lee WY. A mesothelial cyst presenting as inguinal mass: two case reports and literature review. J Current Surg. 2018; 8:38–40.
[3] Kim BM, Lee JY, Han YH, Kim SY, Seo JW, et al. Mesothelial cyst of the round ligament mimicking a metastasis: A case report. Korean J Radiol. 2010; 11:364–367.
[4] Farrands PA, Taylor I. Unusual groin swellings. Postgrad Med J. 1984; 60:309–311.
[5] Harper GB Jr, Awbrey BJ, Thomas CG Jr, Askin FB. Mesothelial cysts of the round ligament simulating inguinal hernia. Report of four cases and a review of the literature. Am J Surg. 1986; 151:515–517.
[6] Ryley DA, Moorman DW, Hecht JL, Alper MM. A mesothelial cyst of the round ligament presenting as an inguinal hernia after gonadotropin stimulation for in vitro fertilization. Fertil Steril. 2004; 82:944–946.
[7] Khanna PC, Ponsky T, Zagol B, Lukish JR, Markle BM. Sonographic appearance of canal of Nuck hydrocele. Pediatr Radiol. 2007; 37:603–606.
[8] Vargas-Ávila AL, Gómez-Montoya LE, Guidos-Gil JC, Ávila-Rivera JL, Huerta-García LD, et al. Quiste de ligamento redondo que simula hernia inguinal encarcelada. Reporte de un caso. Cir Cir. 2017; 85:334–338.
[9] Putzki H, Student A, Mlasowski B, Heymann H. Diagnostic error: incarcerated hernia. Zentralbl Chir. 1986; 111:31–35.
[10] Berná JD, García-Medina V, Guirao J, Madrigal M. Mesothelial cyst of the round ligament. AJR Am J Roentgenol. 1990; 155:1345–1346.
[11] Açmaz G, Aksoy H, Aksoy U, Özyurt S, Esin E, et al. An unusual abdominal cystic mass in the round ligament of the uterus: a case report. J Pediatr Adolesc Gynecol. 2014; 27:e101–e102.