Full Text
Introduction
Majority of the cartilaginous lesions occur in bone. However, many have been described in soft tissues including larynx, synovium etc. Benign cartilaginous tumors constitute about 50% of all bone tumors. These are described in Table 1.
Table 1: Benign cartilaginous tumors.
- Enchondroma – Single / Multiple
- Ecchondroma
- Osteochondroma
- Post radiation and post traumatic osteochondroma
- Multiple osteochondromata
- Paraosteal Chondroma
- Periosteal chondroma
- Epiphyseal chondroma
- Chondroblastoma
- Chondromyxoid Fibroma
- Soft tissue chondroma
- Miscellaneous – Focal, fibrochondral dysplasia,synovial chondromatosis
- Ollier’s dyschondroplasia
Radiological investigations include the following Table 2:
Table 2:
- Conventional
- Ultrasonography
- MDCT
- Pet CT
- Radionuclide scanning
- MRI
All these investigations may not be necessary in all patients. The general principles applied in the diagnosis of bone tumors are given in Table 3.
Table 3:
- Age and Sex
- Single or Multiple Lesions
- Type of Bone involved
- Site of the lesion within the bone
- Site of origin of the lesion
- Nature and extent of bone change
- Appearance of the transitional zone
- Nature of the tumour matrix
- Type of periosteal reaction
- Soft tissue involvement
Diagnosis of chondroid tumours mainly rests on conventional radiology and is made by the anatomical location, transitional zone and mineralization of matrix. The calcified matrix may be minimal or heavy. When there is no mineralization of cortex, it is difficult to make a firm diagnosis. In these instances CT or MRI may be helpful. Endosteal scalloping, thick periosteal reaction and cortical hook when present may add to the correct diagnosis.
Polyostotic
- Multiple enchondromata
- Metachondromatosis (Hereditary)
- Ollier’s dyschondrodysplasia
- Maffuci’s Syndrome
- Multiple osteochondromata
Enchondroma
The incidence is 3-17% of biopsied primary bone tumors. This is the second most common cartilage-containing tumor. It is due to continued growth of residual benign rests of cartilage displaced from the growth plate. It is generally asymptomatic except when there is trauma that result in a pathological fracture (Figure 1).

Figure 1: Enchondroma of fifth metacarpal with pathological fracture.
It commonly presents in subjects between 10 – 30 yrs of age. When multiple these are located in tubular bones of hands (Figure 2).

Figure 2: Multiple enchondromata in the hand.
Multiple enchondromata in the hands is also called Ollier’s syndrome. Other sites affected include long bones including femora, humeri, clavicles and ribs (Figure 3a,b,c).
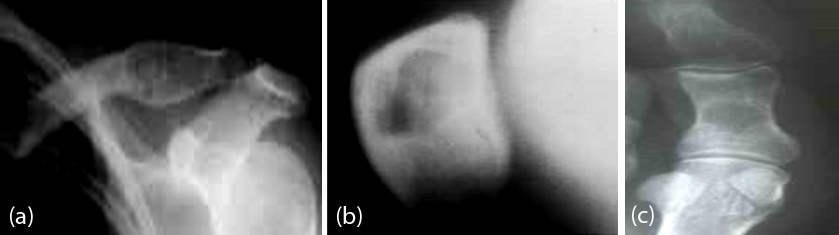
Figure 3a,b,c: Enchondroma in (a) Clavicle (b) Patella (c) Big toe.
Enchondroma is located in the central medullar canal of the metaphysis. The incidence is 3-17% of biopsied primary bone tumors and it is the second most common cartilage containing tumor. The average size is smaller than 3cm. When it exceeds 5cm low grade malignancy should be considered. It is due to continued growth of residual benign rests of cartilage displaced from the growth plate. The calcifications of the matrix may assume the shape of punctuate, arc like, circular, nodular, or a mixture of these (Figure 4a,b). CT shows early mineralization much better than conventional radiography.
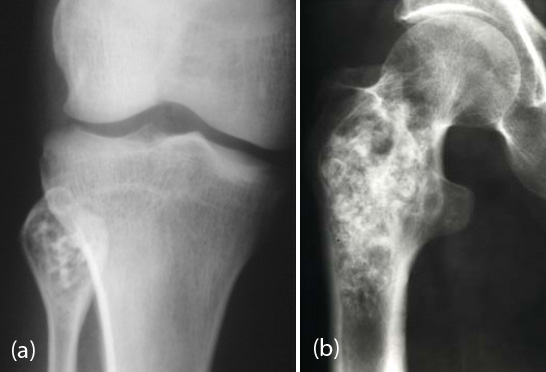
Figure 4a,b: Calcified enchondromata (a) head of fibula (b) intertrochanteric area of femur.
Another finding in cartilaginous tumors is the presence of a hook at the margins (Figure 5).

Figure 5: Intracortical chondroma showing calcifications and the presence of hook inferiorly.
Periosteal chondroma is also called juxta cortical chondroma and is diagnosed by the anatomical location and the presence of calcific matrix (Figure. 6a,b).

Figure 6a,b: Periosteal chondroma in the phalanges with calcifications extending into the soft tissues.
The complications of enchondroma include pathological fracture and malignant degeneration particularly when located in the long-bones whose incidence is between 15 and 20%. In the differential diagnosis, epidermoid inclusion cyst (phalangeal tuft), with history of trauma, unicameral bone cyst (rare in hands, more radiolucent), giant cell tumor of tendon sheath (commonly erodes bone, soft-tissue mass outside bone) fibrous dysplasia (mostly polyostotic) and bone infarct (Figure 7a,b) need to be continued.
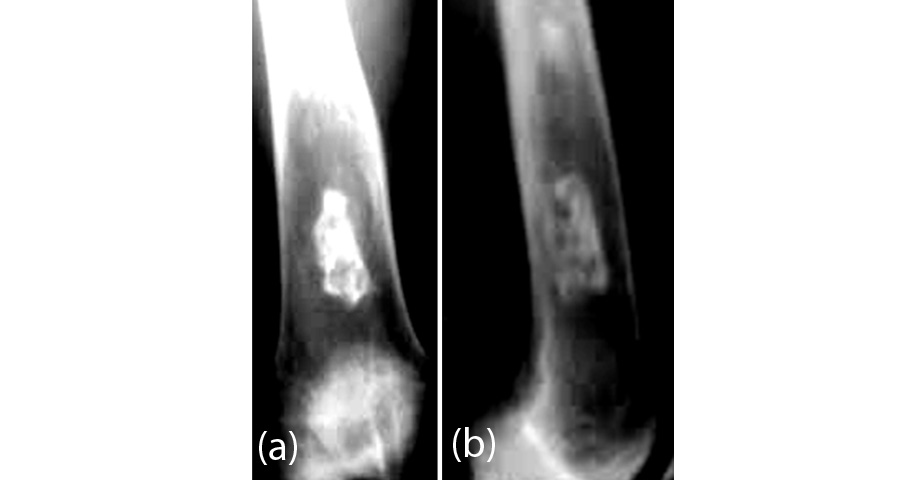
Figure 7a,b: AP and Lateral views of lower end of femur showing bone infarct. Calcification simulates enchondroma.
Maffucci syndrome constitutes multiple enchondromata and soft tissue hemangiomas. It is actually a non-hereditary mesodermal dysplasia. In this connection, an increased prevalence of malignancies in the bone, ovary, duodenum and central nervous system. The diagnosis of Maffucci syndrome is made by the presence of enchondromata and presence of phleboliths in the soft tissue hemangiomas (Figure 8).

Figure 8: Maffuci syndrome. Note the enchondromata and calcified phleboliths in hemangiomata.
Subcutaneous soft tissue chondromas are encountered without the involvement of underlying bones. They show amorphous, lumpy and homogenous calcifications (Figure 9a,b). In occasional, instance calcified soft tissue hematoma and localized Myositis ossificans may be considered in the differential diagnosis.
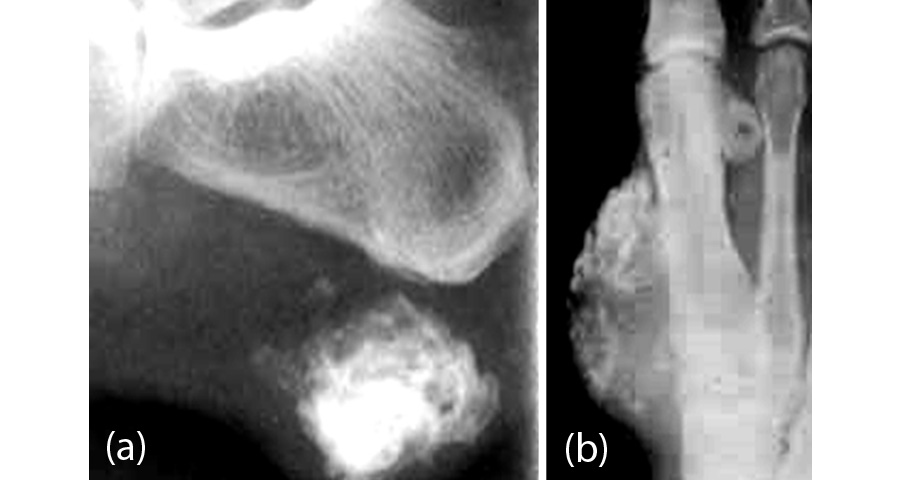
Figure 9a,b: (a) heel (b) hand – Soft tissue enchondromata.
They may be seen in intra and extra articular locations (Figure 10a,b). They may also occur in structures like nasal septum, larynx etc.

Figure 10a,b: Intra articular chondroma of the knee.
Ollier’s dyschondroplasia is a developmental disorder. Chondromatous lesions are encountered in several bones and usually affect children in the age group of 1 to 12 yrs. These lesions are generally distributed on one side of the body. These may lead to shortening of the limb (s). Radiological findings include cortically oriented lesions with calcifications. The hook sign indicates that it is a cartilaginous lesion. This lesion prevents normal growth of the bone and may lead to shortening of the bone (Figure 11a,b).

Figure 11a,b: Ollier’s dyschondroplasia (a) hand (b) femur. Note the hook sign as well as the enchondroma.
Chondroblastoma is a benign cartilage tumor and constitutes 1-3% of all bone tumors. Male and Female ratio is 2:1 and is encountered in 2nd & 3rd decades. Long & short tubular bones are frequently affected. Radiologically a lytic area is noted in the epiphysis or metaphysis, or the lesion may involve both epiphysis and metaphysis. Chondroid calcification is present in 1/3rd of cases (Figure 12a,b).
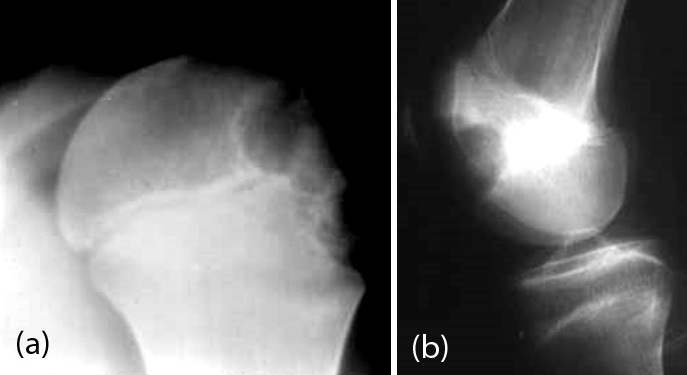
Figure 12a,b: Chondroblastoma in a. humeral head, b. lower end of femur.
When it is primarily located in the metaphysis periosteal reaction may be noted (Figure 13).

Figure 13: Chondroblastoma with periosteal reaction at the base of the fifth metacarpal. Note the pathological fracture.
In about 1/3rd of the cases aneurysmal bone cyst may be associated in which instance, MRI shows fluid – fluid levels (Figure 14a,b).
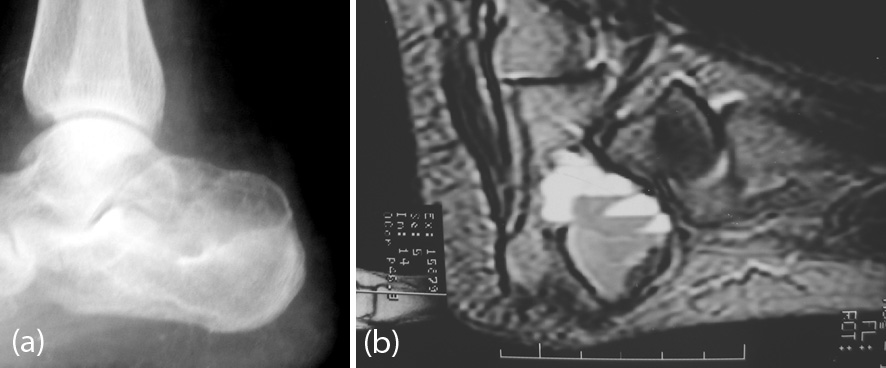
Figure 14a,b: Chondroblastoma of calcaneum. (a) plain film (b) MRI showing fluid – fluid levels indicating secondary ABC.
Chondromyxoid fibroma is a rare benign cartilaginous tumor although it is also included in fibrogenic tumors. It is encountered in 2nd and 3rd decades. It occurs in the metaphysis of long tubular bones as well as short bones of the feet. Radiologically, it is a lytic expanding lesion with lobulated appearance, tending to be eccentric. Trabeculations may be seen with endosteal sclerosis (Figure 15a,b).
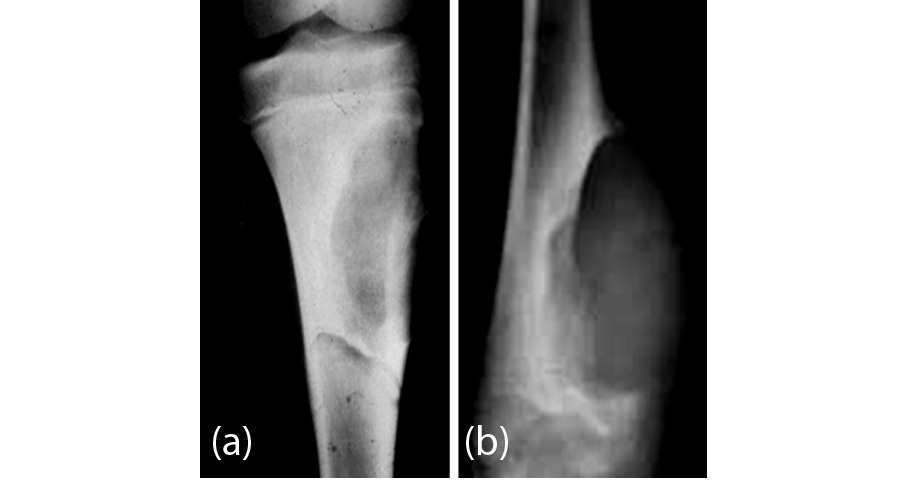
Figure 15a,b: Chondromyxoid fibroma of (a) proximal tibia (b) distal tibia.
This is one of the benign aggressive lesions simulating radiologically an aneurysmal bone cyst. Calcification is rarely noted, although punctate calcifications are noted histologically. Advanced imaging does not really help in the diagnosis.
Solitary osteochondroma (exostosis) is generally encountered in the first four decades. When a single lesion is noted it is appropriate that the whole body is investigated for detecting multiple lesions. Radiologically, it occurs in the metaphysis and diametaphysis and projects out of the underlying bone. It may be sessile or pedunculated. The femora and tibia are the common sitesof its occurrence. The medularic cavity is in continuity of the parental bone. In long bones, these lesions grow away from metaphysis. Diaphyseal eclasis growth takes places in the cartilaginous cap. Growth generally diminishes after skeletal maturity (Figure 16a,b,c). The average thickness of the cartilage is about 2cm.
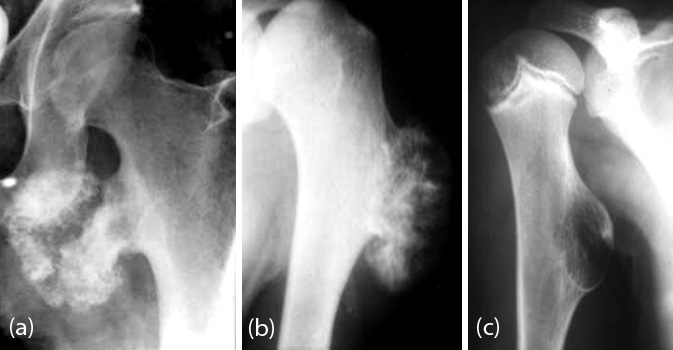
Figure 16: (a) Exostosis of lesser trochanter of femur, (b) Enostosis of humerus. Note cauliflower like osteochondroma, (c) Sessile Exostosis of humerus seen end on.
Multiple osteochondromata (exostoses) are hereditary and autosomal dominant. These are encountered in younger age groups. They are bilateral and often symmetrical. Radiologically, the findings are that of solitary exostosis. However, since they are developmental, shortening and deformity of limbs may be noted (Figure 17a,b,c,d).

Figure 17a,b: Bilateral osteochondromata. Note hook like projections, (c, d) Multiple symmetrical osteochondromata of femur and tibia.
Complications include fracture, bursal formation, compression of nerves and vessels and malignant transformation (Figure 18a,b).

Figure 18a,b: Fracture of the pedinculated exostosis.
In solitary exostosis/ Enchondroma, the incidence of malignancy is ~1% (Figure 19) in multiple exostoses the incidence of malignant transformation may be up to 10 – 15%. In Maffucci syndrome the incidence of malignancy is 20 – 30% which includes non-osseous tumors.

Figure 19: Benign enchondroma undergoing malignant transformation in the lateral aspect eroding the cortex.
Post traumatic exostosis has been described and when its shape is like a tent it is named as Turret exostosis. Another exostosis is due to osteoperiostitis or Nora’s lesion as a sequel to trauma (Figure. 20a,b). Post radiation osteochondromata have also been described.
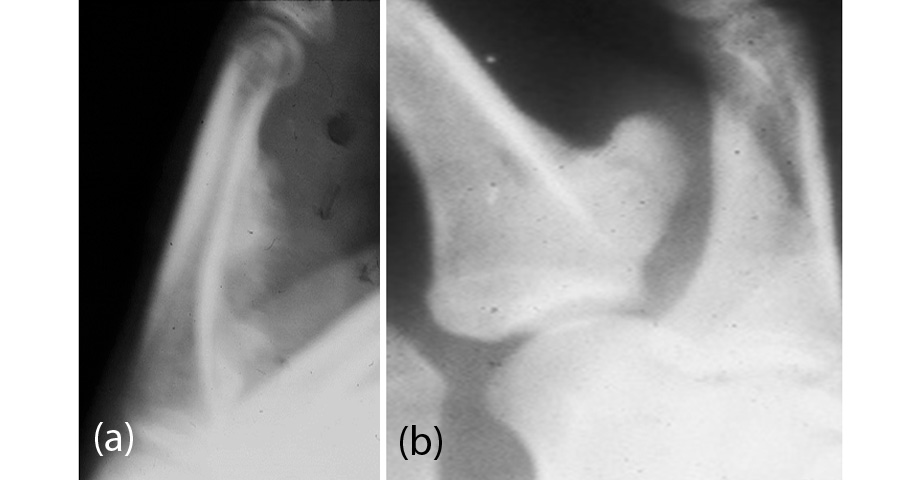
Figure 20: (a) Nora’s lesion due to osteoperiostitis - This is also known as Bizarre Paraosteal Osteochondromatous Proliferation (BPOP), (b) Turret exostosis due to previous trauma.
Trevor’s disease (Dysplasia epiphysialis hemimelica) is a disorder with eccentric growth of ossification centre associated with calcified mass. It may be considered as epiphyseal osteochondroma. This may be hereditary and deformity of joint may develop. Generally, monoarticular but more than one joint may be affected. In this case talus and distal femoral epiphyses are most commonly involved. Radiologically, focal calcifications occur at the epiphysis or apophysis. Affected centres may become hypertrophied resulting in severe deformities (Figure 21a,b,c).

Figure 21: Trevor’s disease involving (a) Femoral head (b) Talus and (c) Knee.
Synovial chondromatosis may be primary or secondary. Primary synovial chondromatosis may be intra articular or extraarticular (Figure 22).
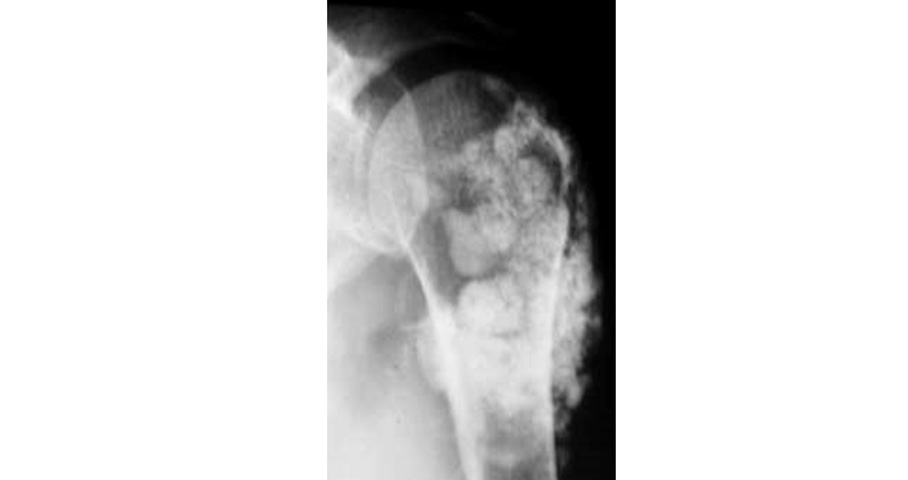
Figure 22: Primary synovial chondromatosis of the shoulder.
Secondary synovial chondromatosis is due to advanced degenerative arthritis. The degenerated and fragmented cartilage and synovium may be separated and form a nidus for secondary synovial osteochondromatosis. Primary synovial chondromatosis is due to metaplasia of the synovium which gets fragmented and nourished by synovial fluid and eventually calcifies and ossifies and form chondromatosis (Figure. 23a,b).
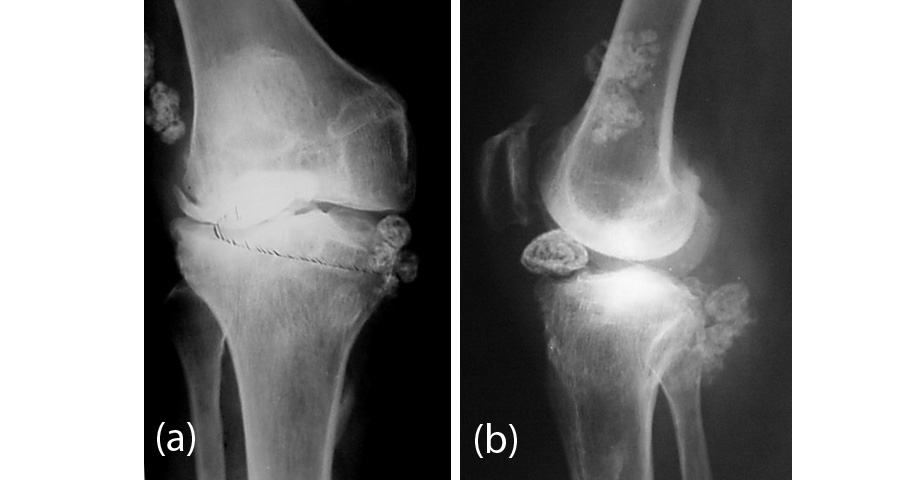
Figure 23a,b: Osteoarthritis with secondary synovial osteochondromatosis (joint mice)
Conclusion
Benign cartilaginous tumors are common and constitute ~50% of all bone tumors. Conventional radiology is adequate enough to diagnose these tumors. Mineralization of matrix in the form of arcs, circles and flocculations is characteristic. Previously, we were the first to describe (7, 8) a “hook sign” in cartilaginous tumors. The classical radiological findings on conventional radiograph are illustrated.
Conflicts of interest
Author declares no conflicts of interest.